
On a warm winter night, a small group of harm reduction workers in Charleston, West Virginia, stuffed the trunk of a gray car with hundreds of kits containing sterile syringes, light blue tourniquets, packets of alcohol swabs, little balls of cotton, and the opioid-overdose antidote, naloxone. All of the ingredients to prevent a fatal overdose and inject drugs without contracting a viral infection.
Before the sun set, this group of mobile harm reduction workers had sent encrypted text messages to people in the area who needed these supplies, detailing times and locations for secret drop-offs. Everyone was told to look out for the gray car.
“We’ve been forced to work in the shadows.”
For the next several hours, I sat shotgun criss-crossing Kanawha (pronounced: Kuh-Naw) County, pulling into parking lots of big box stores and fast food restaurants which, for a brief moment, became sites of health care and civil disobedience. As we arrived at each parking lot, people would approach the car, warily at first. Once the car doors were open and the coast was deemed clear, the hand-offs quickened and people walked briskly away with a word of thanks and their injection supplies.
“It feels like we’re doing a drug deal,” one of the harm reduction workers said, driving to the next parking lot. “We’ve been forced to work in the shadows.”
***
For many people who use drugs, especially in rural states, harm reduction programs function as their only lifeline. Pharmacies refuse to sell syringes. Emergency departments send them home with little more than a brochure of phone numbers. Abandoned by mainstream health care institutions, syringe service programs keep them connected not only to health care, but to kind and caring people.
But that connection has been severed in West Virginia by a state law passed in April 2021. Passing out syringes without explicit approval from state health officials, local commissions and the county sheriff now carries misdemeanor charges, fines of up to $10,000 and possibly jail. For harm reduction programs to operate legally, they must also abide by a strict “one-to-one” rule, which means people can only receive one new syringe for every used one they return. By contrast, the Centers for Disease Control and Prevention promotes “needs-based” syringe programs, which are far more effective at reducing the spread of HIV and other infections. Since the new law took effect, several harm reduction programs have shuttered across West Virginia, leaving vast stretches of the state with no services whatsoever.
The crackdown on harm reduction and the resulting syringe scarcity has been catastrophic for public health. In 2018, only two new cases of HIV were detected in Charleston. But that year, state and local officials decided to shut down a syringe program. By 2020, 40 new people in Charleston who inject drugs were diagnosed with HIV—roughly the same number of new cases as in New York City, which is 47 times more populous. Epidemiologists familiar with West Virginia’s outbreak suggest these numbers are merely “the tip of the iceberg,” and that many more cases statewide have gone undiagnosed and undetected.
In these deserts of care resourceful people and organizations create scattered oases.
The devastation convinced the Charleston group to operate a mobile syringe program without permission, in defiance of the law. They’re taking on immense legal risk, which is why their names are being withheld.

Tents in front of a boarded-up home in Charleston, West Virginia.
West Virginia is far from the only state where harm reduction programs face political, legal and cultural obstacles. Across rural America, programs that distribute naloxone, sterile injection equipment and fentanyl test strips, and which make referrals to low-barrier prescribers of medications like methadone and buprenorphine, are chronically underfunded and struggle to meet the needs of their communities. Meth use, a major contributing factor to rural overdose, remains substantially overlooked. If neighborhood backlash doesn’t drive out harm reduction programs, then councils and state legislatures are more than happy to step in.
Today, demand for harm reduction services across America far outstrips supply and capacity, especially in remote parts of the country where syringe or methadone programs are hours and hours away. Still, rural America contains multitudes, and in these deserts of care resourceful people and organizations create scattered oases. In Charleston, that means breaking the law to distribute supplies to people who drive in from all over the state. Elsewhere, harm reductionists are leveraging online platforms and civic institutions as unlikely sounding as the church.
***
In Kanawha County, one tall woman with bleach-blonde hair was especially grateful for the injection supplies, she said. Earlier in the week she had run out of syringes and resorted to injecting methamphetamine in her neck using an intramuscular needle intended for naloxone, a process she described as horribly painful (the gauge of an IM syringe is far too big for veins).
In a McDonald’s parking lot, a man in his 30s wearing a flat-brimmed New Era hat asked if tonight’s kits had those little blue plastic vials of sterile water. “No, not this time,” one of the workers said, regretfully. The group couldn’t afford to order more water units. In yet another parking lot, the workers handed supplies to a friendly woman named Tabitha, who told all the workers to text her when they got home; like a mom to teenagers, she wanted to make sure they were safe.
“That’s mostly what we’re confronting out here—people’s pain.”
Next, we pulled into a Wendy’s, which was not on the itinerary as an official drop-off site. There we saw two young men slouching on the curb, wearing black zip-up hoodies. The workers offered them supplies, which, it turned out, they needed. One of them, who told me his name was Chris, said, “Everyone’s passing around HIV. There’s no new rigs.”
“Charleston wears its pain on its sleeve,” one of the rogue workers said. “That’s mostly what we’re confronting out here—people’s pain.”
***
Hundreds of vials of naloxone sat on an altar at the United Methodist Church in Columbus, Ohio. The opioid-overdose antidote was due to be blessed in a church service led by preacher and harm reductionist Blyth Barnow. Barnow cheekily titled her service “Naloxone Saves,” a play on the ubiquitous “Jesus Saves” bumper-sticker slogan. Wearing a black dress, she stood at the dais and began preaching the Christian theological basis for harm reduction, connecting naloxone distribution to key concepts like resurrection. This medicine, she said, gives ordinary people great power.
With the lights dimmed, Barnow invited those who’ve lost loved ones to overdose to light a candle in their memory. Across working-class communities in Ohio, where Barnow was born and raised, there are always people in the crowd who have lost family and friends. Overdose deaths recently jumped by 26 percent—to 5,585 lives lost in 2021. Like West Virginia, Ohio’s rate far exceeds the national average.
In the flickering orange glow, Barnow’s voice boomed, “We must step in and help to distribute lifesaving tools like naloxone, fentanyl testing strips, and sterile equipment. We must commit to lifting people up when systems let them fall.” She then read from Matthew, 10:5-8: “Cure the sick, raise the dead, cleanse the lepers, cast out demons. You received without payment; give without payment.”
In each service, Barnow encourages people sitting in the pews to come up to the altar and take as many naloxone kits as they need, for free. “The hope is, whatever naloxone I bring with me that I leave with none,” she said.

Photograph courtesy of Blyth Barnow
I asked Barnow, who is the Ohio associate director for Faith In Public Life, if her strategy was working. Have any churches denied her?
“We had one church that wasn’t comfortable doing naloxone distribution without the health department there,” Barnow said. “So the health department came and distributed [naloxone] based on their protocols and I distributed based on my protocols. The health department distributed 25 Narcan kits and I distributed 75 kits.” Barnow said the health department workers were stunned that she gave away triple what they did. “They had never distributed more than 25 kits.”
“It’s hard to read it as anything other than hate for people who use drugs. Oftentimes, when we get into the nuance, it’s actually people holding a great deal of hurt and grief.”
Health departments in Ohio tend to ask a lot of questions and collect a lot of “data,” Barnow explained, which may make people skittish. Her approach is to make people feel welcome and not ask questions.
“Watching people walk away from the altar with an armful of [intramuscular] naloxone, sometimes taking 25 kits at a time, and seeing that happen in a church sanctuary during a church service, is just deeply meaningful to me.”
Much of her pastoral work, Barnow continued, involves “holding space” and “sitting in the mess” with people while they work through their own internal conflicts.
“A lot of times we see the objections or hostility to harm reduction and it’s hard to read it as anything other than hate for people who use drugs,” she said. “Oftentimes, when we get into the nuance, it’s actually people holding a great deal of hurt and grief that they have never been able to share with another person.”
***
With President Joe Biden in the White House, some had hopes that a landscape hostile to harm reduction would change. For the first time in US history, the federal government included harm reduction as a central tenet of its national drug policy strategy. In another first, Biden’s American Rescue Plan created $30 million worth of grants for harm reduction programs. After decades on the fringes of drug policy, harm reduction was finally being recognized as a valid, necessary and effective approach.
But the recent, albeit partial, embrace of harm reduction at the federal level has often not translated to support at the local level, where America’s streak of punitive, zero-tolerance, abstinence-based drug policy and treatment still holds considerable sway. And that’s particularly true in rural states where conservative values, at least on their face, appear to clash with the practice and principles of harm reduction, which are rooted in self-determination and bodily autonomy. Whereas conservatives prefer people to be self-reliant and free from dependency—in this context, perhaps, “clean and sober”—harm reductionists recognize the importance of interdependence, and try to attach as few strings as possible to help. Few US drug laws have caught up to harm reduction’s view.

Words on a home in Charleston read, in part, “NO SELLING OR BUYING DRUGS ALLOWED HERE LORD HAVE MERCY ON ALL OF US AND USA.”
So often, policy and laws that materially affect the lives of people who use drugs are decided not in Washington, DC, but in city councils, town halls, police departments and the pages of local newspapers. In Alabama, for instance, a new state law prevents telemedicine providers from prescribing a controlled substance unless the patient has had an in-person appointment within the previous 12 months. As a result, rural patients receiving buprenorphine remotely have been scrambling to find a doctor nearby.
In dense urban centers as well as sparsely populated rural areas, harm reduction programs are in the public’s crosshairs— frequently viewed as “enabling” and “coddling” people who use drugs, as prolonging addiction rather than spurring recovery. Harm reduction’s growth has put it on a collision course with America’s dominant paradigms.
“Rural and remote areas are really left out of the harm reduction equation.”
“That’s the climate that we are responding to right now,” said Jamie Favaro, the 42-year-old founder of NEXT Distro, an online platform that sends harm reduction supplies through the mail.
Like the underground syringe program in Charleston, NEXT Distro has found a way to get supplies to those in need, whose numbers have only swelled during the COVID-19 pandemic. Thousands of requests for injection supplies come from people in rural neighborhoods and small towns that lack the services of major metropolitan areas. These locations might be served by just one pharmacy, which may choose to not distribute naloxone, which may not dispense syringes without a prescription, and which might not even stock opioid use disorder medications like buprenorphine. State paraphernalia laws, meanwhile, criminalize the possession of fentanyl test strips, syringes and other supplies.
“Rural and remote areas are really left out of the harm reduction equation,” Favaro told Filter. That’s where NEXT comes in, mailing out the supplies to places without brick-and-mortar syringe programs. The legal assault on harm reduction and public health is perhaps most stark in Tennessee, from where Favaro receives numerous requests for supplies.
“In Tennessee, we call it the ‘Slate of Hate,’” said Lesly-Marie Buer, a harm reductionist and medical anthropologist from Knoxville. “It’s the anti-abortion, anti-trans, anti-LGBTQ legislation that comes up every year.”
This unified conservative caucus invariably targets harm reduction, too. Most recently, Tennessee legislators attempted to require that every single syringe program in the state receive a public written letter of support from local law enforcement. “Let me just tell you, that’s not going to happen,” Buer said. “It would be political suicide for a sheriff or police chief to support harm reduction.”
Out of Tennessee’s 95 counties, only seven are home to legally sanctioned syringe service programs, the majority located in densely populated metro areas. And unlike neighboring states, such as Kentucky, Tennessee has not expanded Medicaid, leaving over 100,000 residents without health insurance and access to critical care. The 10,000 square miles of West Tennessee, in particular, are a harm reduction and health care desert.
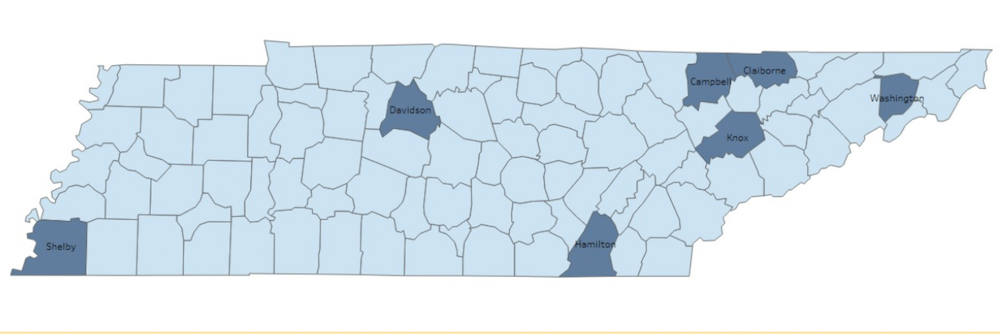
Map of Tenessee counties with syringe service programs via Tennessee Department of Health
In rural Tennessee counties, syringe programs must also be sited 2,000 feet away from any school or park. The state also recently criminalized homelessness, making it a felony for any unhoused person to camp on public land. Critics of the new law say the unhoused population is simply being pushed further from public view, and away from services that could be of help. These barriers on the ground make the work of NEXT Distro all the more salient.
To access supplies through NEXT, people are asked to fill out an “enrollment” form, which helps NEXT assess their needs. One question asks enrollees how often they have shared syringes with another person in the past month. The responses horrify Favaro. “In states like Pennsylvania, West Virginia, Tennessee, Ohio, we’re seeing up to 40 percent of people reporting active syringe sharing ‘all of the time’ or ‘most of the time.’” High levels of syringe sharing, Favaro explained, account for the ever-expanding clusters of HIV and hepatitis C in rural America.
“Never in my lifetime would I think I’d see young people my age dying of HIV.”
“I was 17 years old when I got my first job at an HIV drop-in site,” said Brooke Parker, an outreach worker for Charleston’s Ryan White Program. “I’m 37 now, and never in my lifetime would I think I’d see young people my age dying of HIV.” But, that’s exactly what she is seeing now. Part of Parker’s job is to ensure people living with HIV can access antiretroviral medication, but she cannot offer her clients one of the most powerful tools to prevent HIV from spreading: sterile syringes.
“An increase in acute [hepatitis C] infection in individuals 30 years of age or younger over the past decade has occurred in both nonurban and urban counties,” Dr. Stuart C. Gordon, director of hepatology at Wayne State University School of Medicine in Detroit, wrote in 2019. “But the incidence of infection has been twice as high in rural areas than urban ones.”

A sharps container in Charleston.
Favaro’s voice carried with a mix of sadness and anger over the phone. “Right now, NEXT is receiving about 160 to 200 applications every week for our program,” she said, describing the surging demand as “incredibly overwhelming.” Lacking financial support—NEXT did not win a slice of the $30 million federal pie for harm reduction programs—it’s virtually impossible for Favaro to serve all applicants. NEXT is forced to triage and prioritize only those in severe need. “People just cannot access the supplies they need to be safe,” Favaro said.
***
Blyth Barnow, who identifies as queer, didn’t always have a warm view of religious institutions. She vividly remembers a minister condemning her partner who died of an overdose at their own funeral service. “My friends kept dying and I kept going to awful, awful funerals,” she told me. After years of running away from Christianity, Barnow decided to run toward it. “You’re a shitty pastor, so Imma be the fuckin’ pastor,” she thought. That eventually led to her project to spread harm reduction and drug policy reform through the church, showing churchgoers how their faith actually aligns with these goals.
Her Naloxone Saves service recontextualizes overdose prevention as an act of resurrection, her way of living into the harm reduction maxim of “meeting people where they’re at.” She uses the language, symbolism and principles of Christian theology to engage her faith community around harm reduction, melding worldviews often deemed immiscible, like oil and vinegar. But Barnow views churches across the Midwest as a potential vehicle to preach the gospel of harm reduction.
“I wasn’t born a harm reductionist,” Barnow laughed. “It took some convincing for me.” And yet, “It was through harm reduction that I came to understand that resurrection was a real thing.”
Getting churches on board with harm reduction can be an uphill climb. So is getting harm reduction on board with the church. Barnow attended seminary school in Berkeley, California while working at the Harm Reduction Coalition in Oakland. “I went to seminary as a harm reductionist, as a queer person, as a person raised working class and poor, whose partner was trans,” Barnow said. “A lot of my community has been deeply and negatively impacted by the institutional Christian church and far-right wing Christianity.”
It illustrates how cultures which, on their surface, appear to be hostile to harm reduction can be mobilized to advance it.
So she’s not surprised when people in harm reduction are wary of involving the church in their work. “Like anything, it’s a slow trust-building operation.” Forging that trust has led to thousands of doses of naloxone distributed directly to communities hit hard by overdose deaths.
Barnow’s battle involved changing Ohio laws that placed onerous restrictions on distributing naloxone. Community-based programs seeking to do so required special permission through a Terminal Distributor of a Dangerous Drug (TDDD) license. This posed a major obstacle to scaling up desperately needed low-barrier naloxone distribution.
Barnow organized to change Ohio’s naloxone law by building power between the faith community and grassroots harm reduction organizations. Working together, this coalition slowly made inroads with key groups like the state’s Board of Pharmacy, and then approached state legislators.
In 2020, after years of painstaking work, Ohio’s new naloxone law allowed for more direct, community-based distribution, enabling Barnow to give away hundreds of naloxone kits through churches. It illustrates how cultures which, on their surface, appear to be hostile to harm reduction can be mobilized to advance it.
***
West Virginia, home to “the most concerning” HIV outbreak in the nation and one of the highest rates of hepatitis C, has an overdose death rate more than double the national average. Methadone, proven to reduce mortality among people with opioid use disorder by 50 percent or more, is heavily restricted: Just nine clinics operate in the entire state, forcing people to drive enormous distances to access the medication that could save their lives.
“We have people at the methadone clinic where I go coming from two hours away, everyday,” Mandy Cavender, a 37-year-old resident of Charleston, told Filter. “Some of them pay cash money, $25.50 per day to dose. That’s on top of the gas money to get there. People come from way out there—it’s crazy.”
“Had I just been able to go to the needle exchange and get what I needed, I wouldn’t have HIV today.”
Not long after Charleston shut down multiple harm reduction programs, Cavender learned she was HIV-positive. She believes it could have been prevented.
“Had I just been able to go to the needle exchange and get what I needed, I never would have bought a bag of points on the street and I wouldn’t have HIV today,” she said. “Now I have something I have to live with for the rest of my life.” Cavender is both saddened and enraged by the state’s crackdown. “The cops and the city shut them down so hard,” she said, “which was one of the stupidest things they could have ever done.”
Failure to contain HIV in more urban areas like Charleston has led to its spread in more rural parts of the state. Mountain State Spotlight, an investigative news outlet in West Virginia, reported that new HIV cases were found in 29 West Virginia counties last year, many of them rural and many of which had not seen a new case in years.
“Did you see the McDonald’s right up the street? The little park right next to it?” Cavender asked me. The pitch of her warm Southern drawl deepened. “That’s AIDS Park,” she said. “The walkways made of bricks with names on them. Every one of those names is someone who passed away from AIDS.”
One brick read simply: “In memory of Gary.” Another read: “Garden Friend Edie Maine Ashley.”

Standing on those bricks in the park, the ornate dome of West Virginia’s capitol building looms in the distance. “It’s not a secret, the IV drug use around here is extremely serious,” Cavender said.
I asked Cavender why she thought politicians, law enforcement and parts of the community came down so hard to shut programs dedicated to preventing even more names from being etched into those bricks. Her answer was chilling.
“The amount of homeless people, street people, got really high here,” she said. “It made everything so visible.”
Top photograph of Brooke Parker on her HIV outreach beat and all photographs unless otherwise stated by Zachary Siegel
Correction, August 24: This article has been edited to correct Jamie Favaro’s age.
R Street Institute supported the production of this article through a restricted grant to The Influence Foundation, which operates Filter. Filter‘s Editorial Independence Policy applies.



