
A long white van, stocked with clear plastic cups and a machine that dispenses liquid methadone, was launched in New York City in December. Its purpose is to make methadone more accessible for people with opioid use disorder. Bronx-based VIP Community Services, with funding from the state’s Office of Addiction Services and Supports (OASAS), began doling out doses from what’s called a Mobile Medication Unit (MMU).
It was a long time coming.
In 2007, the Drug Enforcement Administration imposed a moratorium on methadone dispensing vans, citing concerns about potential “diversion.” The DEA offered no evidence to back that claim. It didn’t matter to the drug warriors that the United States was experiencing historic rates of overdose deaths and that getting more methadone to people, especially in rural areas, might save many lives.
“It’s about equity and serving those people who wouldn’t ordinarily, necessarily receive this service.”
Finally in 2021, during the COVID-19 pandemic, the DEA lifted its 14-year ban. DEA regulations still only allow brick-and-mortar clinics to operate mobile medication units.
MMU are intended to address longstanding problems with access. Even in New York City, where there are at least 70 opioid treatment programs (OTP), patients’ travel times can be an hour or more each way. Upstate, where there are far fewer clinics, it can be even longer.
“This kind of initiative is about using harm reduction, bringing services to where people are; it’s about using an evidence-based strategy,” Dr. Chinazo Cunningham, the commissioner of OASAS, told Filter. “We know methadone improves people’s lives. It’s about equity and serving those people who wouldn’t ordinarily, necessarily receive this service.”
Dr. Cunningham said the agency has allocated over $5 million to get MMU up and running. In June 2023, she said that up to 35 vans would be funded and deployed throughout the state, but that number dropped to 11. Two were operational by January, New York Focus reported.
Crucially, the van can induct new people on methadone. This is likely to save lives.
VIP’s MMU currently stops in the parking lots of two inpatient drug treatment programs. Crucially, it not only dispenses medication to people who are already enrolled in methadone programs, but can induct new people on methadone.
This is likely to save lives.
Told it wasn’t possible to observe the van dispensing methadone due to privacy concerns, I toured the empty MMU with VIP staff, as it stood in the parking lot of one of their supportive housing programs.
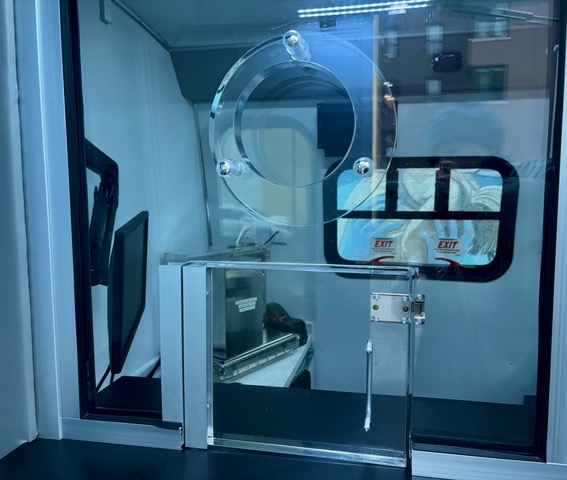
Everything inside was a clean, shiny black and white. There is a space with a table and two comfortable chairs, and an exam room. A locked area contains a dosing window, a computer connected to a methadone dispensing machine, a sink, and a mini safe to store the bottle of methadone.
VIP Community Services operates one of the largest OTP in the Bronx. There, they can medicate up to 1,500 patients per day at nine windows, according to Chief Program Officer Justin Mitchell. “We call [the van] our 10th window, it just happens to be rolling,” he told Filter.
The MMU comes with sticker shock. Originally, VIP was awarded $200,000 to fund it. “When everybody that got the grant started finding out how much a vehicle cost, we all said, no one is going to be able to do this,” Mitchell said. “Then they brought the grant up to $550,000.”
What’s contributing to the expense?
“Security is usually standing right at that door to prevent anybody coming in to see the patient or to prevent the patient from running out.”
“There’s alarm systems for all the doors, there are cameras, both internally and externally,” Mitchell said. “The door to the nurses’ area has its own coded lock so only the nurse has access. The safe is a requirement, it’s a specific type of safe…”

The security requirements go further. Another DEA rule makes patients wait in a separate space from the dispensing area, and the separation must be physical—a door or entryway.
“When we are at a site, security is usually standing right at that door to prevent anybody coming in to see the patient or to prevent the patient from running out,” Joseph McCrawford, VIP’s director of nursing, told Filter. “One of the guys will ride with us all day. He escorts us out to the van with the methadone and escorts us off the van with the methadone.”
To get medicated, a person climbs three steps, goes through a door, and enters a small, private area with a plexiglass dosing window and counter. The nurse opens a small door with a lock to pass through a cup of liquid medication, plus take-home doses.
Policing and surveillance—the guards, safes, cameras, witnessed dosing—are degrading trademarks of methadone clinics, and DEA rules have exported these to MMU.
Vehicles in Porto have no cameras, safes, security guards or plexiglass dosing windows.
That’s in sharp contrast to methadone vans I’ve ridden and reported on in Portugal. Over two decades ago, the country created a national network of vans to bring methadone to neighborhoods with high rates of heroin use and overdose deaths.
Vehicles in the city of Porto have no cameras, safes, security guards or plexiglass dosing windows. Peer workers and a nurse load the van with a bottle of methadone and other supplies, then drive to a designated location. The door is opened wide and a nurse sits on a cushioned bench with the methadone dispenser and cups. People often hang out and chat with staff, creating the feel of a mellow tailgate party.

This low-key, friendly way of dispensing methadone is the opposite of what the DEA’s methadone security state imposes.
Besides security, the VIP MMU is also staffed with a driver, a nurse, a doctor, a client care coordinator, and a peer support specialist.
Currently, the program partners with two inpatient drug treatment providers—Phoenix House in Queens, and Odyssey House on Ward’s Island—to deliver methadone. VIP is also seeking to partner with nursing homes to deliver methadone going forward.
Currently, about 50 people are registered to receive methadone in the MMU.
At each stop, about 15 to 20 patients are seen, and typically they get a week of take-home bottles. “They bring them into the facility and give them to the nursing staff and it’s held in their department,” Mitchell said.
While some recipients are already enrolled at VIP’s OTP, others enroll for the first time at the MMU. Some are enrolled at other clinics, but receive “guest dosing” from the van as they attend residential treatment.
No urine screens are done on the van, though participants are subjected to them elsewhere. “We’re taking the toxicology reports that the residential programs are doing and we scan them into our electronic medical record,” McCrawford said.
Currently, about 50 people are registered to receive methadone in the MMU. The van dispenses methadone three days a week, from around 9 am to noon. “We’re usually back to home base around 1:30. Then we do all the reports,” McCrawford said. “We have to make sure the count is correct, that what we have on hand matches the count in the safe. If it does, we had a great day.”
But are MMU in this form the most efficient and financially feasible way to get methadone to large numbers of people during an unprecedented overdose crisis? The answer is no.
Outreach to areas where people are using fentanyl is precisely what the van ought to be able to do.
To be sure, dosing people in the parking lot of their rehab or nursing home offers convenience, which really matters when travel times are so disruptive to people’s lives. And the ability to induct new patients represents a critical, though very limited, expansion of access.
Clinics also appreciate partnerships with treatment programs because onsite medical staff will store the medication, alleviating unfounded concerns about safety and diversion.
“If you wanted to serve people who are street homeless, it would be harder to go every day, or go with the frequency that they would need to be able to manage their medication safely,” Mitchell said. “I mean, that’s always a thing, right? How many bottles can you give someone that they can manage and store safely?”
But that kind of outreach is precisely what the van ought to be able to do. The mission, according to Commissioner Cunningham, is about equity and offering methadone to people who “wouldn’t ordinarily receive this service.” That includes people who are unhoused and living on the street.
The Bronx has the highest rate of overdose deaths in New York City. The MMU should park in areas where people are using fentanyl and offer methadone there, seven days a week. That level of access would do more to bring down overdose deaths.
But the exorbitant costs of maintaining MMU even part-time are not sustainable for most OTP. On a recent webinar, I heard an OTP employee criticize the focus on methadone vans on this basis: “There is a reason so many clinics and hospitals are selling mobile units. When the grants run out, you sell the van.”
A grant funded the startup costs for VIP’s MMU, but won’t pay for ongoing operating expenses which include at least four employees, supplies, fuel, insurance and vehicle maintenance.
“We have to generate revenue, so when someone comes to the window, we’re billing a dispensing rate,” Mitchell said. “We have to have clients that we’re billing for in order to generate the revenue.”
What happens if there aren’t enough insured patients dosing at the van, and sufficient revenue isn’t generated? Unfortunately, odds are good that in the future, MMUs like this could be auctioned off for a pittance, or sit gathering dust as half-million dollar write-offs.
Their existence can only be seen as minimal progress in the context of our inexplicable failure to implement pharmacy dispensing of methadone.
There are further problems with MMU as they stand. When they only visit a restricted number of locations, it’s still a hardship to travel to one.
And their existence can only be seen as minimal progress in the context of our inexplicable failure to implement pharmacy dispensing of methadone, like in the United Kingdom and Australia. No other medication is only available in a siloed, carceral clinic system.
MMU participants surely appreciate not having to attend a brick-and-mortar clinic—and definitely benefit from accessing methadone when they couldn’t have done so without the program.
But would anyone who uses other medication choose to take it under the watchful eye of a nurse, in a guarded vehicle in a parking lot? Would we have a similar birth control pill pop-up truck, Ritalin RV or Viagra van? No! It’s simply not a dignified setup.

Despite the positive efforts of OASAS and VIP, MMU are not a sustainable big-picture answer. They’re ultimately an inefficient way of getting methadone to a large population in the midst of a crisis that has killed over a million people.
The answer is that any health care provider should be able to write a methadone prescription in a wide variety of settings—syringe service programs, shelters, encampments, overdose prevention centers, street medicine outreach teams, drop-in centers—with pharmacy pickup or delivery.
There are 2,600 pharmacies in New York City alone, and over 5,000 in New York State. MMU will never be able to expand access on that scale.
Photographs by Helen Redmond



