
Between stigma and bureaucratic challenges, accessing methadone and other medications for opioid use disorder (MOUD) can be an uphill battle at the best of times. But for many people in the United States, physical distances and travel times between where they live and facilities that offer MOUD are huge additional barriers.
Experts say that the notion of service “deserts” can also be applied to syringe programs and other harm reduction resources. And the issue is widespread.
New research out of Ohio State University flags the existence of “opioid treatment deserts.” And while people living in rural areas are often particularly vulnerable, the paper identifies numerous such areas within the state’s capital city.
The researchers first began working on the project in 2015. The team gathered overdose data from first responders, notably Columbus’s fire department, for the years between 2013 and 2017: 6,929 overdose events in all. From there, they created maps of locations with high instances of overdoses that were also a good distance away from the city’s 22 MOUD providers, both by car and by public transit.
Reaching methadone treatment took much longer: three times longer by car on average, and 2.5 times longer by public transit.
Within the paper, deserts are defined as areas in which overdose events occur that are either 1 mile away by car, or 30 minutes away by public transit, according to coauthor Harvey Miller, a professor of geography and director for the Center of Urban and Regional Analysis at Ohio State University.
The research—part of a larger project called the Franklin County Opioid Crisis Activity Levels (FOCAL) Map—assumes that the overdoses reported through the first responders mostly occurred in peoples’ homes, but Miller noted that’s not a perfect metric. The distances set in the paper to define an opioid treatment desert are also not perfectly defined, he said. Rather, the paper introduces the concept and shows how to measure it.
Regions further from the city’s core or main thoroughfares tended to have longer travel times and distances, and more parts of the city were identified as deserts when taking public transit over cars.
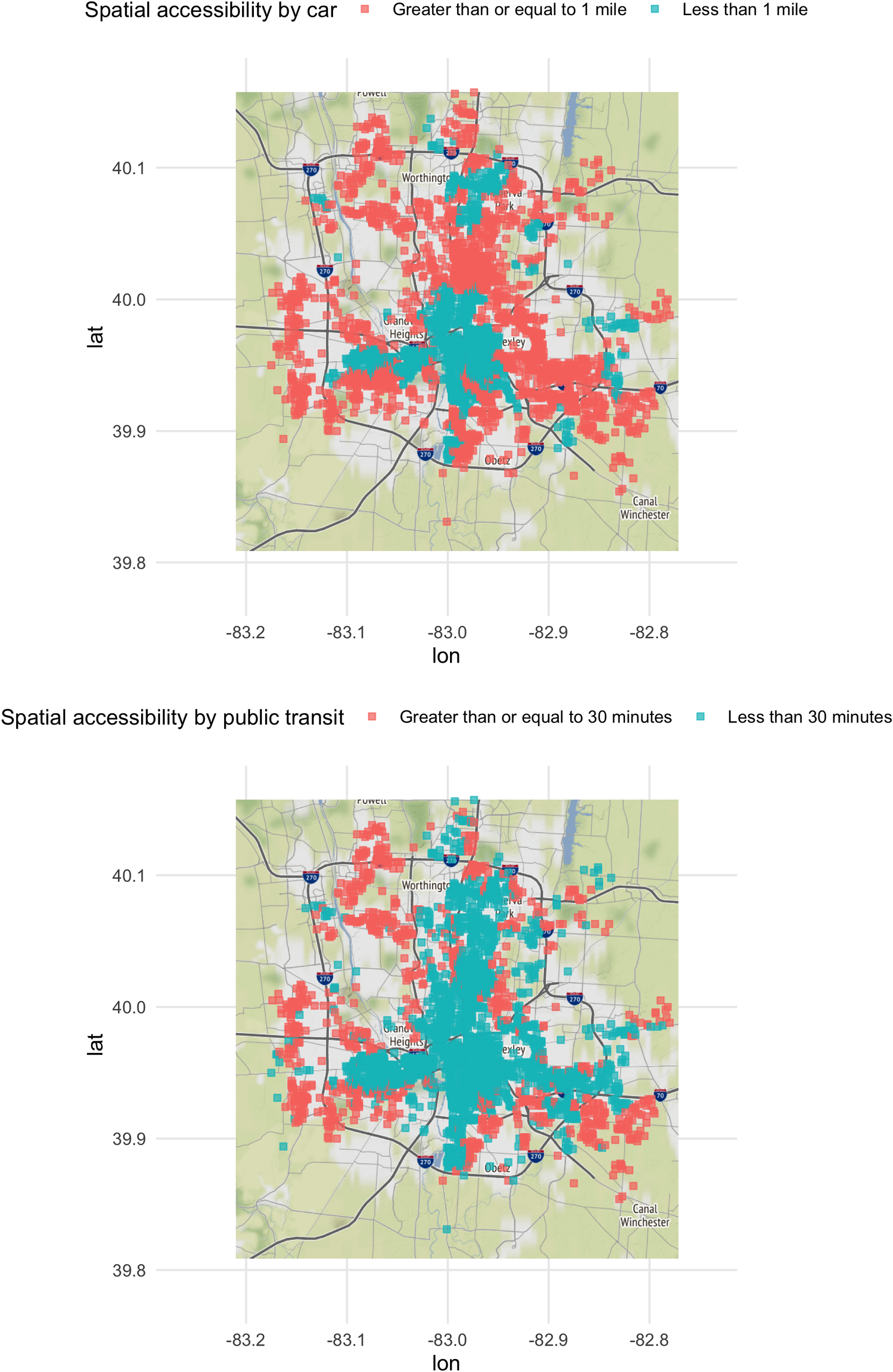
Maps of Colombus produced by the study, with neighborhoods deemed “opioid treatment deserts” in car and public transit terms shown in red. © 2021 Hyder et al, originally published by PLOS ONE. Creative Commons 4.0
“We think there needs to be more empirical studies on what the correct travel time threshold is—whether by car or public transit,” Miller told Filter, adding that success rates in methadone or other treatment increase with accessibility.
Access times also varied depending on the form of MOUD concerned, the paper found. The median travel times to reach a MOUD facility were two minutes by car, and 17 minutes by bus. But reaching methadone treatment specifically—which can only be provided by a certified Opioid Treatment Program, or methadone clinic—took much longer: three times longer by car on average, and 2.5 times longer by public transit.
That’s particularly onerous—potentially to the point of being unmanageable—when many methadone patients are required to attend clinics almost daily.
Columbus is not alone in this. It’s likely that there are other cities that sprawl more and have fewer treatment programs, just as the inverse is also probably true. “Columbus is a very typical city in America,” Miller said, adding that the methods outlined in the paper could also be extended to apply to a range of other harm reduction facilities.
Texas: “Everything’s Just So Far Here”
According to Aaron Ferguson, a member of the Urban Survivors Union’s leadership team, much of Texas, where he lives, suffers from a lack of treatment and service options, with large distances between those providers that do exist.
“In that case, all of Texas would be considered a treatment desert,” he told Filter. “To make a blanket statement, I would say a very small percentage of Texas is not a desert.”
Cities in Texas tend to sprawl over large areas and, in part because of a culture of driving, there have not historically been large investments in public transit, Ferguson said. Meanwhile the traffic in some of these cities can add a long time to any trip. The matter only gets more complicated in rural areas, where finding an MOUD provider or harm reduction service might mean driving to another municipality.
“Everything’s just so far here,” he said.
“Generally speaking, meeting people where they’re at is a better strategy than getting them to a clinic.”
Cate Graziani, co-executive director of the Texas Harm Reduction Alliance, said that cultural factors also contribute to difficulties in accessing these facilities. Harm reduction, as a concept, is largely stigmatized; Ferguson said that part of this is because there’s a long history of abstinence-based and 12-step programs within the state.
Graziani noted that there are some underground harm reduction organizations in Texas, but very few official options, despite a syringe service program in Bexar County becoming the first to operate legally in the state. Pre-pandemic, a state representative also filed a bill that would make it legal for community groups and churches to run syringe programs, local media reported.
Mobile harm reduction operations could help reduce some of the negatives of deserts, however. For instance, Graziani’s organization—partly due to the pandemic—does a lot of outreach work in Austin. They go to around 15 encampments set up by homeless people per week, giving out harm reduction supplies and working to connect people with methadone and buprenorphine providers, she said.
“Generally speaking, meeting people where they’re at is a better strategy than getting them to a clinic or a facility,” Graziani told Filter.
Though Graziani and Ferguson are based in Texas, their involvement in wider harm reduction networks means they’re well aware of other deserts across the country. Ferguson noted that these are quite common in Middle America.
Dana Saltalamachia, a community health outreach worker with lived experience of drug use, has resided in many places across the US, including Louisiana and Mississippi, and knows what it’s like to live in places where the nearest services are many miles distant. Now based in Austin, Texas, she said that she’s formerly lived in rural areas where the nearest hospital—never mind methadone clinic—is an hour away.
“It makes it hard to live a normal life, you know?”
Having previously accessed MOUD, Saltalamachia noted that the challenge of physical distances in rural areas is far worse when your only options are to walk or take a bus. When she lived in Waynesboro, Mississippi, the nearest MOUD provider was around an hour’s drive away, in another town.
“There are more barriers. It’s extremely difficult,” she told Filter.
Like others, Saltalamachia noted that the challenges of harm reduction deserts compound other barriers that exist everywhere. With buprenorphine, for example, the X-Waiver requirement for prescribing doctors, even if it was recently eased, caps patient numbers and limits providers—increasing the chance that patients will have to travel further to find what they need. “I think we need to make it more available, and make it more affordable,” Saltalamachia said.
As for methadone, some clinics Saltalamachia has known offer only a four-hour window each morning during the week for people to access their medicine—an even bigger inconvenience when your need to travel long distances makes it harder to time your arrival. “It makes it hard to live a normal life, you know?”
“Food deserts,” and “health care deserts” have become well established concepts in discourse around inequality. Yet right now, treatment or harm reduction deserts remain relatively under-researched, though there are some drive-time studies available.
Miller said he hopes that other researchers will take the approach that he and his coauthors adopted and apply it to other cities, because identifying treatment deserts could be used to find the best places to open new facilities in the future.
“I would suspect [deserts are] possible in almost every American city,” he said. “Even in compact cities, if movement’s an issue because of public transit or traffic, it can still happen there.”
Update, June 24: This article has been edited to clarify the definition of “deserts” used in the Ohio State University study.
Photograph of Big Bend National Park in Texas by Yinan Chen via Wikimedia Commons/Creative Commons 1.0 Public Domain




{kind=link}