
At Washington Corrections Center (WCC), in Shelton, WA, opioids are an increasingly large part of the drug supply. But though our correctional officers (COs) have access to Narcan, the common branded version of the opioid-overdose antidote naloxone, many are not properly trained to use it. They are also actively discouraged from learning.
Two COs told Filter that if someone appears to be overdosing, they won’t administer Narcan because it doesn’t work on fentanyl.
A third said that his Narcan training didn’t include anything about rescue breathing, just chest compressions.
A sergeant said that though officers present during an overdose or other medical emergency are required to respond, they are told verbally—as part of their training—that if they don’t feel comfortable administering Narcan, then it’s better to not intervene at all. The other officers also characterized this as an unofficial but widely known loophole. All requested that they not be identified for this article.
Narcan is effective at reversing the respiratory depression caused by any synthetic or organic opioid, including fentanyl. It usually works after one or two doses. It’s increasingly common to hear stories of people being brought back with three or more doses; but it’s rarely clear whether that many were actually needed, or whether they were simply administered without waiting the full two minutes for the first ones to kick in. During that time, the victim almost never needs chest compressions; they need you to breathe for them.
Though the parameters of Washington State Department of Corrections staff Narcan trainings aren’t completely clear, it’s common knowledge that many officer trainings come in the form of videos that are not interactive or accompanied by any sort of knowledge test. COs are frequently seen playing them on mute, during their shifts, while talking to their partners and going about their other duties. WDOC did not respond to Filter‘s request for comment by publication time.
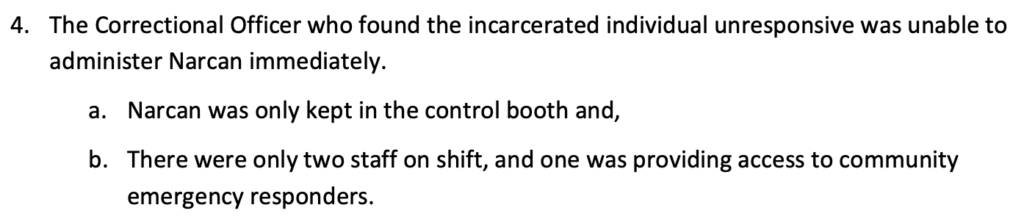
WDOC is required to submit Unexpected Fatality reports for accidental prisoner deaths like overdoses. Several reports from within the past year describe staff at the scene of an overdose not knowing where their facility’s Narcan was located, not knowing how to use Narcan, or both.
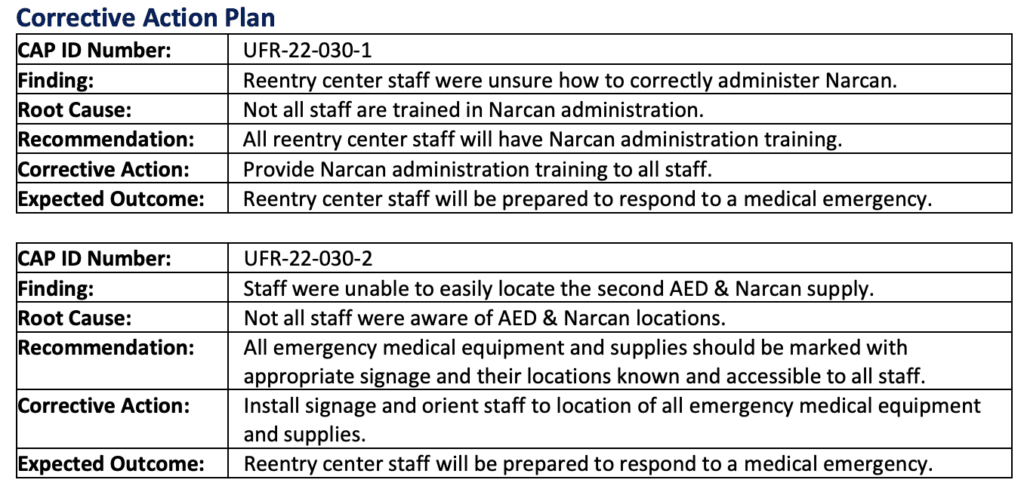
“The Sergeant’s office was identified as a Narcan storage location, but responding staff were unable to find it in the emergency,” reads a report from December 2022. “When Narcan was brought to the scene, responding staff were unaware of how to administer it expelling some of the container’s contents attempting to understand how to administer the substance.”
That report describes officers administering three doses of Narcan, without clarifying whether rescue breathing was also administered, to a man later pronounced dead from lack of oxygen following suspected fentanyl overdose. The report advises officers that for future situations, “[d]ue to the potency of fentanyl being found in the community, using a single dose of Narcan is inadequate.”
Some of the officers reached by Filter attributed their aversion to using Narcan to the perceived threat of wrongful death lawsuits. It’s their understanding that if they intervene at all, they must do so according to certain standards or else be potentially liable if the person they’re assisting doesn’t survive. It’s common here for officers to state unequivocally that they will not intervene in any kind of medical emergency, from an overdose to a heart attack. They will simply call medical and wait for them to handle it.
Medical often responds promptly, but is not guaranteed to. Partly because WCC is physically divided into three isolated sections, and partly because medical is not sufficiently staffed to respond to more than one emergency at a time.
During a security drill in late March, a mock assault was staged in the education building and medical was called in to treat a prisoner who was “unresponsive.” Please be advised, we heard over the intercom, medical staff has never been to the education building and does not know where it is.
Each of the main officers’ stations in each of the main buildings has at least one clearly marked Narcan box. Prisoners don’t have access to them. Since Filter wasn’t able to view their contents it’s not clear whether some or all included masks—a standard component in Narcan kits, but just for hygiene purposes. But multiple officers expressed to Filter that they were unable to perform rescue breathing without masks. The sergeant added that they do have access to the personal protective equipment masks brought in during COVID, but those aren’t kept with the Narcan.
Though it’s been a long time since I used drugs, I still recall how cops would tell me that if I ever needed CPR, they wouldn’t do it unless they had a breathing mask—because I have HIV. Many others have likely been told the same thing, because they’re Black, or Brown, or trans, or they use fentanyl.
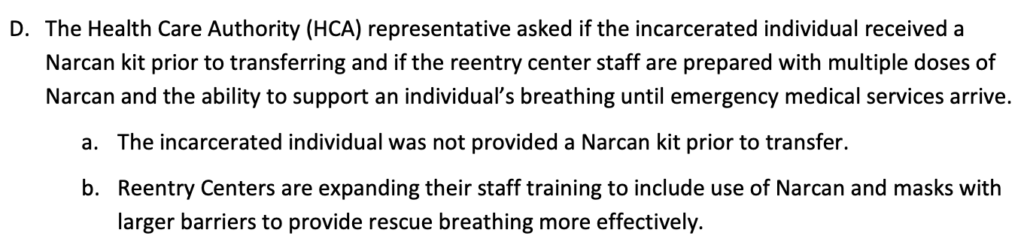
A report dated April 7 stated that among other corrective actions that had already been implemented, Narcan was being offered to prisoners upon release and “[r]eentry center staff now carry Narcan on their duty belts.”
One person, who was recently released and more recently brought back, confirmed that he did receive a Narcan kit on his way out. “Reentry center staff” refers to all WDOC employees at transitional centers; these do not include WCC, so Filter was unable to confirm whether Narcan appears on duty belts at those facilities as of April 7.
In many US prisons, opioids aren’t prevalent in the drug supply the way they are in the free world. WCC, however, is the intake facility through which all Washington state prisoners are processed from county jails before they’re transferred to wherever they’ll be housed long-term, so there’s significantly more movement in and out than is typical for state prisons. And though opioids have always been around, since the onset of the pandemic we’ve seen a steady influx of fentanyl—the blues—to the point that it’s now nearly as prevalent as the methamphetamine that’s long dominated WCC supply.
Law enforcement has a much longer reach than harm reduction programs, and many people who use drugs get their harm reduction education from cops. Out of approximately 20 currently incarcerated people who spoke with Filter, all of whom have been using opioids long-term, 12 expressed that even if they had access to Narcan, they probably wouldn’t bother with it because they heard it wasn’t strong enough for fentanyl. Most were surprised to learn that it is, and that Narcan usually comes with step-by-step instructions.
Top photograph, first inset image, second inset image, and third inset image all via Washington State Department of Corrections



