
It’s legal for adult use in 19 states, two territories and DC, and for medical use in 37 states, four territories and DC. It’s on the Nasdaq, and produced in a capitalist profusion of brands and formats. Despite not being legal everywhere yet, cannabis and its derivatives are increasingly considered part of “wellness” culture.
This is reflected by increasing research focus on benefits rather than harms. Meanwhile, 108,000 Americans died from overdoses involving other drugs, primarily illicit opioids, last year. Given the prominent (though far from exclusive) role of opioids in the current drug poisoning crisis, there is naturally great interest from policymakers, researchers and investors in the possibilities of cannabis in addressing both perceived and real harms around opioid use.
I’ll say right away that I have a personal stake in this. I’ve tried both a prescribed synthetic cannabinoid and a variety of regular cannabis preparations through Canada’s medical cannabis program, in hopes of finding a readily accessible alternative to effective but stigmatized opioid medication for the management of my pain from ankylosing spondylitis, a degenerative spine disease.
Ultimately, however, a low dose of an atypical opioid has proven to be the most tolerable treatment to restore my function and quality of life over more than a decade. I have not experienced opioid use disorder (OUD).
But what does the research say? It was long near-impossible to study cannabis in the United States (and challenging elsewhere). Yet over the past couple of decades, research on the drug has grown. As a result, data pointing to the potential of cannabis or its constituents to reduce opioid-related harms have increased, and—given the way in which such harms increasingly frame research questions—continue to accumulate.
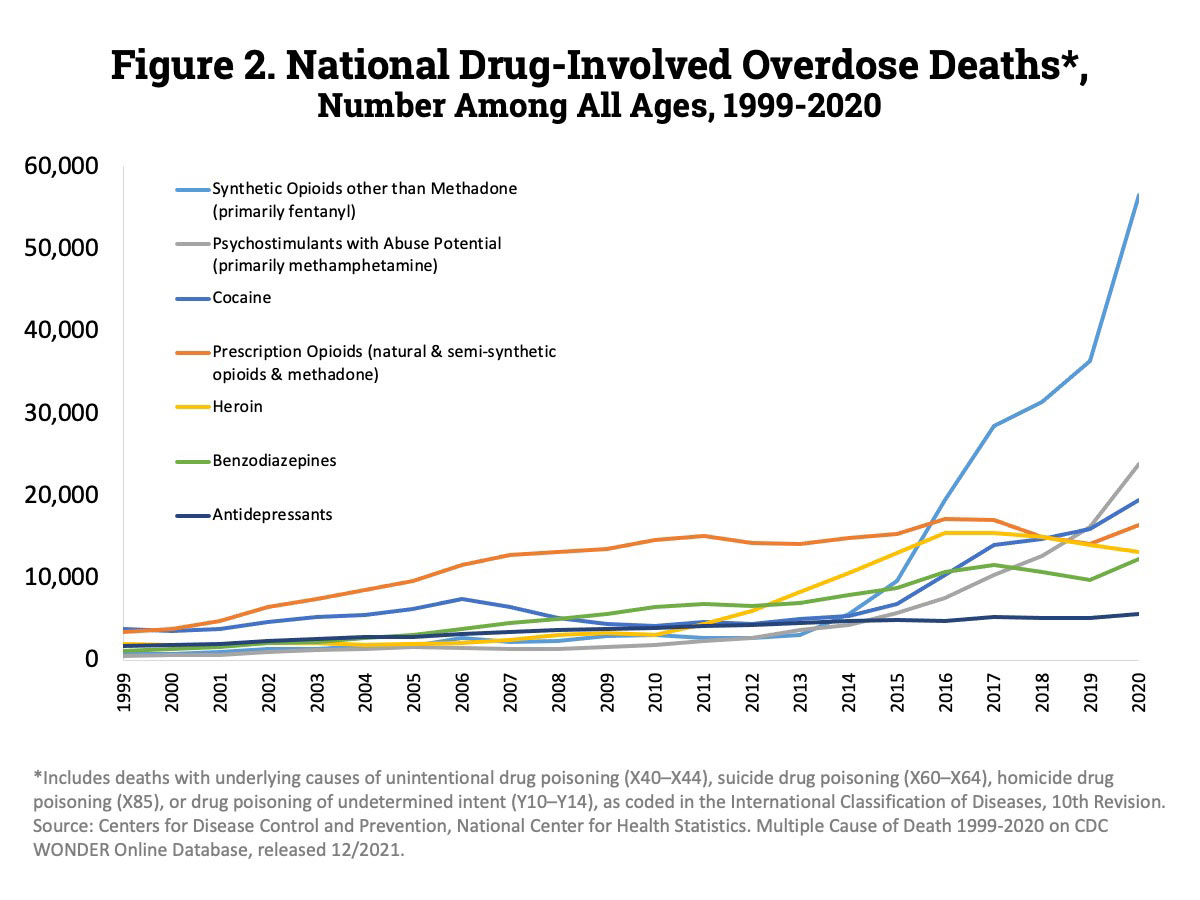
Prior to 2010, access to legal cannabis did seem to prevent overdose, but as opioid use shifted from prescription drugs to heroin and then fentanyl, this became less relevant.
In sorting through this literature, it’s important to tease out conflicts of interest and wishful or ideological thinking that color the framing of studies and the conclusions that may be drawn. Nevertheless, there are many good things to say about the increasing availability of cannabis in a society where both pain and anxiety are rife.
Indeed, there has been hope that cannabis legalization and decriminalization may already be having an organic effect. A 2014 review of death certificates and medical cannabis laws in all 50 states between 1999 and 2010 found significantly lower rates of opioid-involved deaths in states with medical cannabis laws.
When this study came out, its exciting findings—at a time when, as now, overdose deaths were skyrocketing—received significant media attention, and it has been cited by hundreds of other research papers since.
Later studies, however, have seriously muddied the rosy picture in which cannabis straightforwardly replaces opioids and all harms are reduced. One review, for example, showed that by extending the study period of the 2014 paper, the negative association between medical cannabis laws and opioid-involved overdose mortality lost statistical significance.
That is, prior to 2010, access to legal cannabis did seem to prevent overdose (and admissions for opioid painkiller addiction treatment), but as opioid use patterns shifted away from prescription drugs to heroin and then illicit fentanyl, this became a less relevant protective factor.
Most recently, a 2022 case control study and individual-level data review simply found no such protective association between fatal opioid-involved overdoses and state medical cannabis laws. There is a profusion of more local data, though, and it’s rarely studying exactly the same thing in the same way over the same time period—and often seems contradictory.
A 2017 study, for example, concluded that adult-use cannabis legalization resulted in a small monthly reduction in opioid-involved overdose deaths in Colorado, but a 2020 study of this relationship over a longer time period found inadequate evidence to say that adult access to cannabis reduces opioid-involved deaths.
There’s potential in the increasing availability of cannabis for reducing opioid-related harms—if we can figure out the right policies.
When it comes to medical cannabis use, the ways in which it may influence opioid use and overdose clearly depend on many ever-shifting factors. And yet, more experimental and mechanistic research, as well as anecdotal reports, suggests continuing potential in the increasing availability of cannabis for reducing opioid-related harms—if we can figure out the right policies and practices to take advantage of it.
“People almost exclusively talk about the quality of life being better on cannabis than opiates,” Peter Grinspoon told Filter. He’s an addiction medicine doctor well-known for both his medical cannabis advocacy and his openness about his own past experience of prescription opioid addiction (he’s written a book about the latter; a second book, looking at data on cannabis in historical perspective to address common misconceptions, will be published next spring).
Dr. Grinspoon outlines four ways in which he says cannabis can help: to start new chronic pain patients on cannabis rather than either opioids or non-steroidal anti-inflammatory drugs, which can have severe side effects especially with long-term use; to (voluntarily, he specifies) transition chronic pain patients from opioids to cannabis; to use cannabis in conjunction with opioids to treat pain disorders; and to treat opioid withdrawal.
Each of these is indeed a possibility—although the first two, in particular, are controversial among harm reduction advocates and pain patients—and it’s worth examining the data supporting each of these uses of the much-redeemed drug.
Before Trying Other Drugs for Pain
While few people die of overdose from opioids prescribed to them for pain, there is a theoretical risk of accidental overdose as well as a real risk of suicide by overdose in this population, to which I belong. Then, although illicitly obtained prescription opioids could be seen as protective if they replace a dose of heroin or illicit fentanyl of unknown potency, many people who use non-prescribed opioids actually do so to treat physical pain, and are at higher risk of harms, including overdose, than “official” patients.
The risk is that in the enthusiasm for cannabis or the rush to avoid opioids, a patient is denied fair treatment.
Long-term effects of opioids—such as reduced androgens like testosterone and consequent risk of bone thinning, as well as tolerance and physical dependence (which can also arise with chronic, heavy cannabis use but is less problematic)—might also be avoided by never starting them in the first place.
It’s because of this that opioids are very rarely considered a first-line treatment for chronic pain; typically, a patient will first have been asked to try non-pharmaceutical and at least one and probably more non-opioid pain medications. Such pain treatments, often taken for long periods, include non-steroidal anti-inflammatory drugs (NSAIDs), which may come with serious long- and short-term side effects.
Cannabis works on a different body system from opioids, but with many overlapping effects; most notably, analgesia (killing pain) and anxiolysis (killing anxiety). While opioids bind to the mu-opioid and other opioid receptors, triggering a cascade of biochemical effects on the brain, gut, and other parts of the body, cannabis triggers the endocannabinoid system, which, just like the endogenous opioid system, produces self-made chemicals similar to the active molecules of cannabis.
Cannabis has a notable benefit over opioids: there is no risk of respiratory depression, and overdose death is essentially impossible. If it were possible to get equivalent analgesic and anxiolytic effects from cannabis, it would therefore be generally far safer for people using opioids, especially illicit opioids, to treat mild-to-moderate (not severe) pain, unless they have potential contra-indications, such as (for example) high risk of heart attack or schizophrenia. If a well-tolerated dose of cannabis isn’t effective, the patient might then and only then consider NSAIDs or opioids.
The risk of advocating this, of course, is that in the enthusiasm for cannabis or the rush to avoid opioids at all costs, a patient is denied a fair trial of opioid pain treatment even when it best balances the risks, benefits and individual values of that person. Caution is warranted.

Transitioning Pain Patients From Opioids to Cannabis
Tyler Prock, a 37-year old Texan, told Filter that he moved to Colorado in 2012 to gain access to medical cannabis after he was prescribed two opioids (tramadol and hydrocodone) and another painkiller to deal with pain from scoliosis. Although he was only on opioids for two weeks, his personal psychological experience with them was negative, yet his doctors expected he would continue with them indefinitely.
After what Prock described as terrible opioid withdrawal (“It was worse than any hangover I’d ever experienced with alcohol”), and six months of experimentation with cannabis products to find the best type, dose and route of administration for them, he has not looked back. He mentioned that his wife’s autoimmune disorders, for which she had tried a variety of medications, also seem to be under control thanks to five daily dabs of cannabis.
“I was just lucky that I had a friend introduce me to cannabis before [opioid use disorder] would be an option,” Prock said.
(A 2018 meta review found incidence of opioid use disorder among long-term pain patients of just 4.7 per cent including all studies; about 3.1 per cent if only “good” quality studies are included; and approximately 0.2 per cent among patients with no prior history of substance use disorder.)
Besides obvious variations in individual preferences and tolerances, different types and intensities of pain respond better to cannabis than others. Esther Choo and colleagues (2018) note that evidence on the use of cannabis to treat pain is limited by the number and quality of studies, and by the difficulty of drawing useful conclusions for patients given the wide range of cannabis strengths, compositions and preparations available.
While evidence validates its use for certain types and intensities of pain, it has been promoted far more widely and it is prescribed for any number of indications. Of course, it’s not unusual for a drug to be prescribed for “off-label” uses; but if it is pushed without adequate evidence on patients who were stable on a given type and dose of opioid, they may be risking hard-won stability on the basis of wishful thinking.
Even if not coerced, patients fearing opioids might avoid seeking the best-evidenced treatments.
In New York State and Illinois, laws were amended in 2018 to allow patients with an opioid prescription to access cannabis instead. Although it offers welcome flexibility for patients who want to try cannabis, some commentators warn that in the process of encouraging what is increasingly seen as an innocuous, “natural” panacea as an alternative to opioids, more effective but more stigmatized alternatives are being underprescribed, including methadone and buprenorphine (well-evidenced treatments for people with OUD and for some people with chronic pain). It could also, perhaps, increase stigma for patients who choose to stick with opioids.
In cases of opioid cravings in patients who believe, rightly or not, that they cannot access opioid treatments, an unsuccessful experiment with cannabis could be fatal if they then resort to the illicit opioid market. In developed cannabis markets like Canada and legalized US states, marketing often emphasizes myriad supposed medical benefits.
Even if not coerced, patients with fears around opioids, whipped up by overdose headlines and politicized crackdowns on prescribing, might avoid seeking the best-evidenced treatments and instead self-medicate with cannabis for conditions for which it doesn’t work, risking reduced function as well as overdose.
Dr. Ziva Cooper, a researcher who studies cannabinoids at UCLA, also warns of the limitations of survey studies that self-select for people who have had positive experiences with cannabis use for pain being generalized to others, and of the need for research to better determine who might benefit, and how.
Given evidence that the opioid crisis doesn’t substantially involve opioids prescribed for pain, it seems unlikely that replacing pain treatment with cannabis will prevent overdose deaths.
As a Co-Treatment With Opioids
The notion of offering cannabis as an adjunct treatment to patients who are already prescribed opioids is well founded, however. When pain patients have access to cannabis, they often voluntarily reduce their regular opioid dose. Given that patients often require higher doses of opioids over time due to the development of tolerance, even maintaining a constant dose with the help of cannabis can be considered a victory that could reduce the likelihood of opioid side effects.
Dr. Cooper has been working with colleagues on the experimental use of sub-therapeutic doses (too low to be expected to help with pain, and too low to trigger side effects) of the opioid oxycodone in combination with smoked cannabis THC, to see if the synergistic effect can provide adequate pain treatment with fewer negative effects. This was an attempt to build with placebo-controlled human studies on still poorly-understood interactions that have been found between opioid (mu-opioid) and cannabinoid (CB1) receptors.
“There’s overlapping behavioral and physiological effects of drugs that act at these two receptors,” Cooper told Filter. “If you have an animal that is opioid dependent, so they’re receiving opioids daily, and then you take the opioid away, just like with a human being, you’ll see opioid withdrawal symptoms. If you then give that animal a drug that acts as a CB1 receptor, like THC, you will see a reduction in that withdrawal, and vice versa.”
Cooper’s team found the same in their volunteer human population—although Cooper warns that this was experimentally-induced acute pain in a non-pain patient population of existing cannabis users, a highly selected group for the highly controlled study. More human research is needed to say whether the same results might be found with other forms of cannabis, a complex pain patient population, or a population with experience of opioids and no experience of cannabis.
Is the association because it reduces pain? Because it eases opioid withdrawal? Or because it helps with stress, or insomnia?
An important 2019 study of people who use illicit drugs in Vancouver, where opioid-involved overdose rates have been extraordinarily high, compared drug users with chronic pain who used cannabis with a similar population of drug users, also with chronic pain, who did not. It found that daily cannabis users had about a 50 per cent lower likelihood of using illicit opioids on any given day than those who didn’t use cannabis, suggesting that daily (but not occasional) cannabis use has an opioid-sparing effect for chronic pain.
Other research has shown the same. Dr. Stephanie Lake, lead author of this study, notes it did not prove that cannabis can work as a direct substitute for opioids, however. “Now we need to figure out what is driving the association,” she told Filter. Is it because it reduces pain, for example, because it eases opioid withdrawal, or because it helps with other symptoms associated with pain, such as stress or insomnia?
A law similar to Illinois’ that makes it possible for people to access cannabis in addition to their methadone, buprenorphine or chronic pain opioid treatment—and that makes it illegal to kick someone out of treatment for using cannabis—could be a sensible idea that’s well supported by evidence.
To Treat Opioid Withdrawal
The most contentious assertion about cannabis in relation to opioids is that it can function as a direct replacement for a person who is physically dependent on opioids and going through withdrawal. Preventing withdrawal is vitally important for people with OUD who are very likely to resort to illicit opioids to treat unbearable symptoms; it is also important for the medical stability of pain patients physically dependent on opioids.
It’s important to be clear on the high risk of overdose if a person tries to treat withdrawal with cannabis, finds it ineffective, and resorts to a dose of illicit opioids. Or where internalized shame about the use of opioid agonists or “meds” instead of “natural” remedies like cannabis could result in a dependent person pushing themselves to rely on cannabis even if it is not adequately preventing withdrawal.
There have long been anecdotal reports from people who find cannabis helpful in easing specific withdrawal symptoms. “I can say personally that it was extremely helpful for my withdrawal symptoms,” Grinspoon said. “Cannabis works to so many different neurotransmitter systems to [just] the endocannabinoid system that it really is spectacular for opiate withdrawal symptoms.”
Indeed, rates of cannabis use are high among people initiating medications for OUD, especially during the period before dose stabilization. However, in a 2020 systematic review of 43 studies involving methadone, buprenorphine or naltrexone treatment for OUD and cannabis use, Stephanie Lake and her colleague Michelle St. Pierre discovered most studies did not in fact find a statistically significant relationship (either positive or negative) between cannabis use and treatment outcomes, except for withdrawal where evidence at least suggests it doesn’t hurt.
“In general what I found in that review was that the evidence was very mixed,” Lake said. It would “support working with someone using cannabis to find out why they’re using cannabis.”
Chris Backer, in Halifax, Canada (following High Hopes, a more established program in the Downtown Eastside of Vancouver), supplies free “care packages,” including a variety of donated cannabis products, to people who use illicit opioids. Backer’s East Coast Cannabis Substitution Program is a volunteer program not backed by any independent medical organization (Backer had an association with Direction 180, a Halifax opioid treatment program run by the Mi’kmaw Native Friendship Centre, but said that the medical director withdrew due to a perceived conflict of interest).
“We have spectacular evidence for the efficacy of buprenorphine and methadone. With cannabis we don’t have that data.”
Backer told Filter that the roughly 200 people to whom he and other volunteers hand out the kits, with the goal of facilitating a move off of opioid use, are all experiencing addiction. Backer cited some of the evidence mentioned earlier, and said that providing as much cannabis as possible enables people to reduce the number of shots (heroin or fentanyl) they do each week. He said that he has no concerns about a possible heightened risk of overdose due to abruptly reduced opioid tolerance in a highly dangerous market.
Grinspoon, however, distinguishes between easing withdrawal during treatment with buprenorphine or methadone, and actually attempting to replace these drugs, which he warns is not supported by the literature—yet.
“From the perspective of a doctor, we have spectacular evidence for the efficacy of buprenorphine and methadone, a 50 per cent decrease in overdoses and deaths,” he said. “And with cannabis we don’t have that data.”
The risk of overdose if it doesn’t work is high, he added. “I really do think cannabis should be viewed as an adjunct in this capacity.”
Research Is Still Playing Catch-Up
Gateway theory supposes that the non-medical (or perhaps even medical) use of cannabis can increase the likelihood of moving on to other drugs and ultimately to opioid use disorder. This used to be received wisdom but has now been widely debunked.
The sheer numbers of people using cannabis for both medical and non-medical reasons without concomitant increases in opioid use would seem, in itself, to put paid to the idea. Yes, studies have shown that cannabis use, and particularly heavy cannabis use, often precedes use of other drugs. But that doesn’t demonstrate causation, and is akin to saying that people who use drugs are more likely to use (other) drugs.
Evidence to date seems to support the notion that cannabis should be made more available as one option for patients as part of a hierarchy where a trial of cannabis might be recommended before opioids for certain patients and conditions. It also supports the contention that using cannabis, along with well-evidenced medication-based opioid use disorder treatment, should be considered a legitimate version of recovery from OUD rather than a reason to get kicked out of one’s treatment program.
Despite roughly 20 years of accumulating data, it seems that in some respects cannabis research has not yet caught up to the ways it is enthusiastically used, and in others, clinical practice has some catching up to do. With time, science should provide us with data to better define the ways in which cannabis may indeed act as an “exit drug” for opioids, and where its use is not borne out by evidence.
Top photograph courtesy of elsaoloffson/Pixabay. Inset photograph of Tyler and Samantha Prock courtesy of Yaka Jefferson
R Street Institute supported the production of this article through a restricted grant to The Influence Foundation, which operates Filter. Filter‘s Editorial Independence Policy applies.




{kind=link}