
Every drug user I talk to regularly has heard my case for putting drugs up your butt. It’s a conversation that doesn’t work in certain settings, but if you have some privacy even the warier folks often express some level of interest.
The most common complaint I hear is that someone tried it and it didn’t work. But over time, the more people I talked to both in person and online, a few other patterns have emerged: that boofing was too much of a hassle; that it took too long; that it hurt.
This gives me anxiety. All those descriptions are valid in the sense that they’re all relative, but not relative to injecting or smoking. Boofing should be faster and simpler than injecting or smoking, about on par with sniffing and second only to swallowing. It should not hurt at all.
People who are introduced to boofing in a social way, like chemsex or conversations with friends, aren’t usually the ones reporting these problems. The reason I never experienced them is that in early 2021, prior to which I was mostly smoking (mostly meth), comrade Sessi Kuwabara Blanchard gave me a little boofing care package and we had a nice talk about it, and since that day I have never looked back.
The disconnect seems to happen more when people are introduced to boofing through their local syringe service program (SSP). A lot of SSP do distribute boofing kits, but there’s not always much overlap between the people who make them and the people who use them. With that in mind, the following are suggestions for making better kits—using only the supplies SSP already have—as well as talking about boofing’s utility as a harm reduction tool.
Syringes
The best thing to boof with is a syringe that doesn’t have a needle. SSP boofing kits I’ve come across use the 25g blue tip syringes, the Luer lock kind with the needles you can twist on and off. The 25g is the size that straddles the range of larger needles suitable for injecting hormones into muscle or tissue, and smaller needles preferred for injecting drugs into veins. But, in my experience at least, they’re very rarely used for the latter and therefore SSP don’t tend to run out.
The shape of a Luer lock tip is not an intuitive or efficient or comfortable thing to put in your butt.
Respectfully, the blue tips do not make good boofing syringes. Just because a syringe is designed for the needle to come off does not make it good for boofing. Blue tips are just the default SSP boofing syringes because they’re the only Luer lock ones many programs distribute.
The shape of a Luer lock tip is not an intuitive or efficient or comfortable thing to put in your butt, and the 3ml barrel attached to the 25g is three to six times bigger than what most people are used to. This combination makes it difficult to get the full dose where it needs to go. Particularly for people using opioids, this can mean a bad enough experience that they don’t bother to try again. (Anything you can dissolve in water or is already liquid you can boof, although I would not recommend doing it with things like GHB or liquor. It will hurt.)
This could be regional or otherwise skewed by personal experience, but I’ve never been to a well-resourced SSP that didn’t also have stacks of BD 28g and 29g syringes sitting around. These are very cool for the few people who get the hang of the BD needles and despised by everyone else, and lots of SSP just sort of have them around for times of drought.
The needles on the BD .5cc syringes aren’t interchangeable like Luer locks, but they are detachable, kind of. Once you prise off the plastic cover that holds the needle, what you’re left with underneath is a much better shape for boofing than a Luer lock.
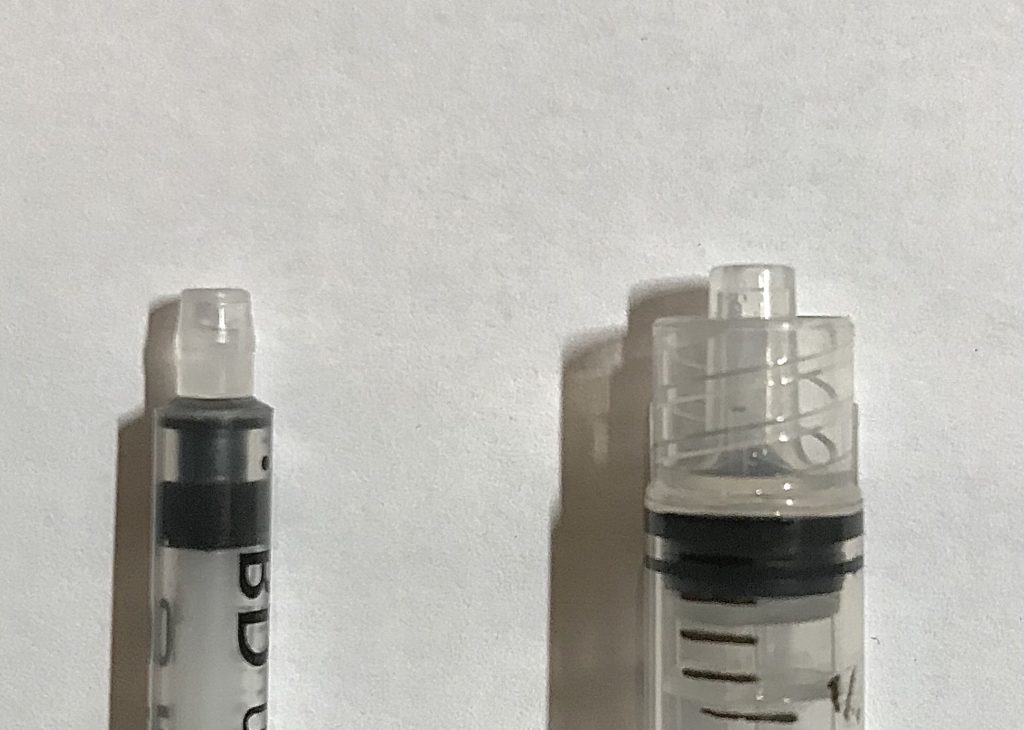
Left: BD 28g .5cc syringe with plastic cover removed. Right: BD 3ml Luer lock syringe with detachable 25g needle removed.
Bend off the needle (dispose safely) and then put the orange cap back on. Bend the tip back and forth, slowly, working your way around so you’re bending evenly on all sides, until the dome-shaped part separates from the syringe. Sometimes the plastic is brittle enough that the whole tip of the syringe will snap off; this is still usable if you don’t have any spares. If you have a small-ish pair of pliers, you can skip all that and just pull everything off in one go.
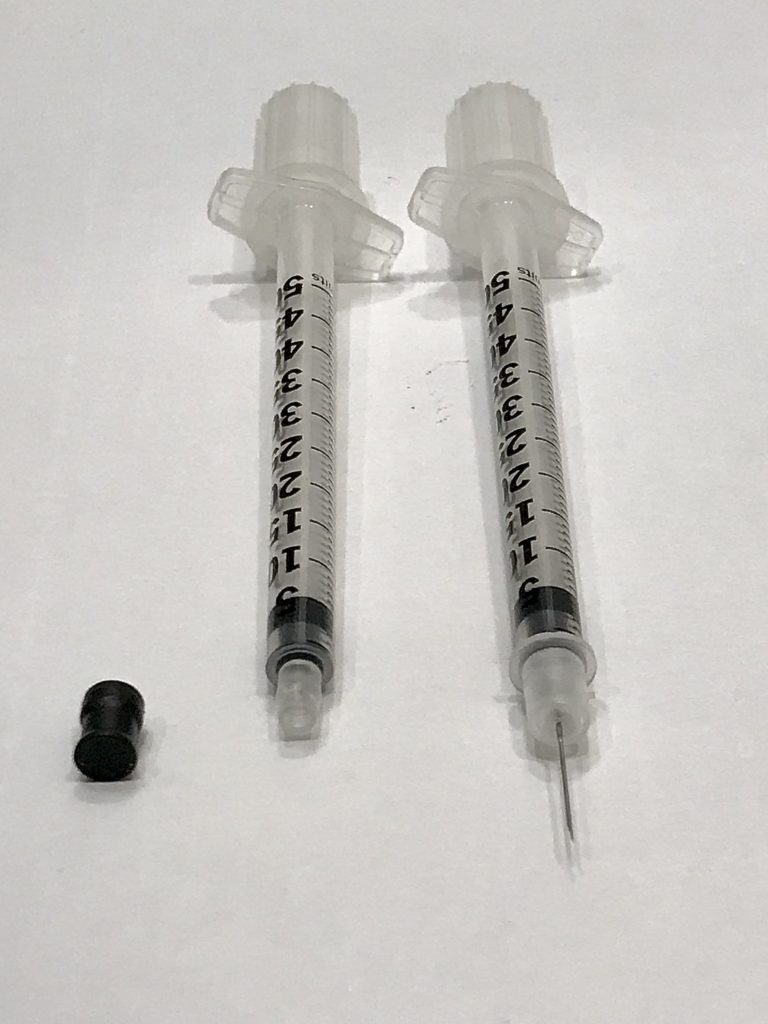
These .5cc syringes also let you eliminate dead space in the tip. Pull the plunger back two or three units before you draw up, and you’ll just have airspace stuck in the tip once you’re done; not drugs. This doesn’t really work with the 3mL barrels—they’re too big to hold pressure in the same way, so the air bubble tends to slide around, and the tips already have about twice the dead space as the .5cc syringes anyway.
Without exception, boofing had not worked for them because they thought the syringe is supposed to go, like, fully up your butt.
You can pull the needles off the BD 28g 1cc, or any other syringe made by any other brand, and still use it to boof. But the tips on other common SSP orders have those pokey ridges, and a boofing kit with a syringe that is a friendly shape has the best odds of actually being used. But the ridged kind are still viable if you need them to be—boofing is much gentler process than many people assume.
Whenever someone tells me they tried boofing and didn’t get anything out of it, it’s an easy fix. Without exception, 100 percent of the time, boofing had not worked for them because they thought the syringe is supposed to go, like, fully up your butt.
It’s supposed to go about half an inch up your butt. You’re aiming for the tissue just inside the rim, which will absorb things into your bloodstream. Any deeper and you’re just kind of shooting the drugs into space.
Insert just the tip of the syringe, then depress the plunger very slightly—do you feel the coldness (or lukewarmness) of the water, the way you would if it was on your skin?
If you feel the water, you’re in the right place; proceed with the rest. Try a test shot with just water if you don’t want to risk wasting anything. This is best, and also only, technical skill there is to learn about boofing.
Modifications
Start to finish, boofing takes maybe two minutes once you get the hang of it. But most of that is waiting for your drugs to dissolve. For situations where you don’t have the luxury of much time or privacy, you can cut the process down to about 10 seconds by pre-loading a syringe and being mindful of how you carry it so the plunger stays in position. (With the BD syringes especially, make sure the plunger isn’t pulled back past the cc lines or it becomes annoyingly prone to falling out.)
You can make a cap by taking the rubber seal off the plunger of any 1cc syringe. It’ll fit over any .5cc or 1cc syringe, including the blue tips. It’ll also fit over an opened Addipak sterile water vial so you can get multiple uses out of them rather than one, which only took me several hundred vials drying out at the bottom of my backpack to realize. If you’re using stimulants, or opioids that you don’t need to heat, you can just use the plastic plunger cap as a cooker and pretty much have an all-in-one product.
Myths and Stigma
Even in harm reduction circles, talking about boofing elicits a subtle but unmistakable suspicion wherein people really want to find something wrong with it, in a way I have never experienced when talking about other injection alternatives. Not just from medical professionals, but from drug users too. People will chime in that they’re not so sure, that they’ve heard something about how in the long-term it rots your colon, or something like that.
Some people I’ve had the boofing conversation with had previously had been told that for it to work properly, they needed to lie down and leave the plunger in for at least 20 minutes. One had been told an hour. Some had been told that if they boofed more than a few times, or more than a certain number of times within a certain number of days, they would get tears in their anal tissue.
Boofing in a chemsex setting, or otherwise just boofing and having unprotected anal sex, can cause tearing that can subsequently put you at increased risk for HIV transmission. But some people had simply been told boofing increased their HIV risk, but not given any context as to why, or at least not in a way that they remembered.
If the whole thing was less noticeably homophobic I’d have my doubts too, because boofing really does feel like cheating. Drug consumption methods tend to have risks and benefits that are proportional to one another: Intravenous injection has 100 percent bioavailability, and is also the highest-barrier to do safely. On the other end of that spectrum is oral consumption. Smoking and sniffing fall somewhere in the middle.
Boofing is the most potent way to use drugs other than injecting them, and it’s faster and easier and safer and more portable and discreet than everything except taking a pill. The only real inconvenience is that if you have not pooped recently, boofing (especially stimulants) works like a suppository, so it’s not a great idea without an accessible bathroom. But you can do it sitting or standing or however you want, and you don’t have to leave the plunger in or do anything else after you’re done.
I boof anywhere from maybe three to eight times a day. So in total—best guess—somewhere between 2,000 and 3,000 times, pretty much consecutively. I wouldn’t be surprised if long-term boofing does involve complications that will reveal themselves to me at some point, but that’s even more true of injecting or smoking or sniffing. The only way to not find out is to stop using drugs, which like many drug users I have no plans to do.
Boofing is a pretty workmanlike route of administration. You’ll never miss. You don’t need steady hands. You’ll always get it on the first try.
Boofing is a pretty workmanlike route of administration. There’s no artistry or intuition or expertise to acquire. You’ll never miss. You don’t need steady hands. You’ll always get it on the first try. It will always take the same amount of time.
We don’t really do people any favors by framing boofing as a replacement for injecting. Regardless of whether boofing provides sufficient effect, that approach devalues the attachment many people have to the physical ritual of injecting. It’s more useful to frame boofing as an option—especially for situations where injecting is risky or isn’t working.
Because we associate syringes with needles, it’s understandable to fall into the familiar talking points we use for injecting—sterile water, sterile syringes, new syringe every time, filter out particulates. It’s not wrong to approach boofing this way, but it’s not necessary for the process to be safe and effective.
While it’s not advisable to share boofing syringes, you surely can reuse them. It’s actually better harm reduction to suggest that people do hang onto them, to be sanitized and stored in whatever way makes them feel not icky. Folks aren’t exactly picking up a whole box at a time.
If someone has access to sterile water and wants to use it, they should of course do so. But we need to frame this as a matter of personal preference rather than a form of harm reduction, because it serves no one to take a perfectly good form of harm reduction and make it seem more complicated than it actually is.
When someone doesn’t have sterile water to inject with, they’ll do it with blood or urine or the rain water we’re not even supposed to drink anymore. Those are harmful because they’re going in your veins, which makes any situation when someone doesn’t have sterile water a very good time to boof. The water doesn’t have to be sterile. It doesn’t even have to be water. You don’t have to filter out impurities. It’s going in your butt.
Photographs courtesy of Kastalia Medrano



