Thanks largely to Gabor Maté, it has become popular to say that addictions are overwhelmingly rooted in trauma.
However, the data do not bear this out. Some people with addictions have co-occurring post-traumatic stress disorder—and PTSD rates are much higher in this group than in the general population—but the majority do not.
Living beings have a limited behavioral repertoire to respond to infinite possible environmental stimuli. In physics, we try to find a single cause for many different effects, like the law of gravitation. In biology, however, the same response is typically elicited by many different stimuli. Flight, for example, is one common biological response, but there are countless different things we may run from.
We are all different, and trying to reduce all addictions to a single cause does us a great disservice as humans.
Substance use disorder, similarly, can have many different causes. For some people, it has its roots in trauma—but for others it’s depression or anxiety, and for others still, the causes do not lie in any co-occurring disorder. We are all different, and trying to reduce all addictions to a single cause does us a great disservice as humans.
Let’s look at a number of major data sources, which measured their findings in quite different ways, to see what they tell us about addiction and co-occurring mental health disorders, which we’ll abbreviate as CMHD.
First, we’ll take SAMHSA’s annual National Survey on Drug Use and Health (NSDUH). NSDUH does not measure different mental health conditions individually, and probably fails to catch personality disorders. But it includes a general measurement of psychiatric impairment based on depression, anxiety, etc.
The survey for 2021, which we’ll focus on, had 69,850 subjects. It found that a little under half (44 percent*) of people with any substance use disorder had CMHD. However, rates varied greatly: Just under 40 percent of people with an alcohol use disorder had CMHD, whereas that applied to almost 55 percent of people with a drug use disorder (involving any drug, pharmaceutical or illicit, other than alcohol).
Interestingly, the Epidemiological Catchment Area (ECA) study, conducted from 1980-1985 with 20,291 subjects (19,182 survey completers), showed very similar rates. It found that 37 percent of people with an alcohol use disorder had CMHD, compared with 53 percent of people with a drug use disorder.
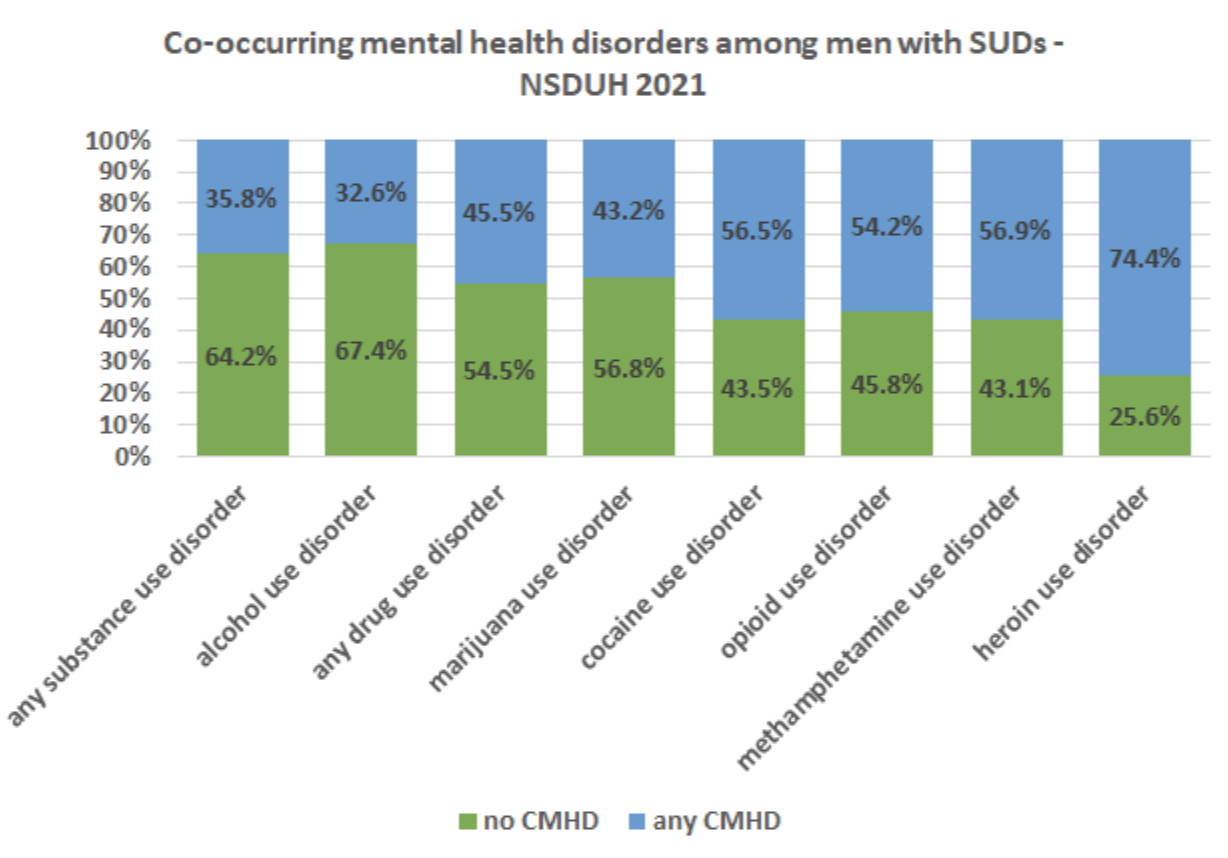
Returning to NSDUH, we find striking variations between individual drugs. For example, almost 75 percent of people with a heroin use disorder had CMHD. I’ve illustrated the numbers in the graphic below:
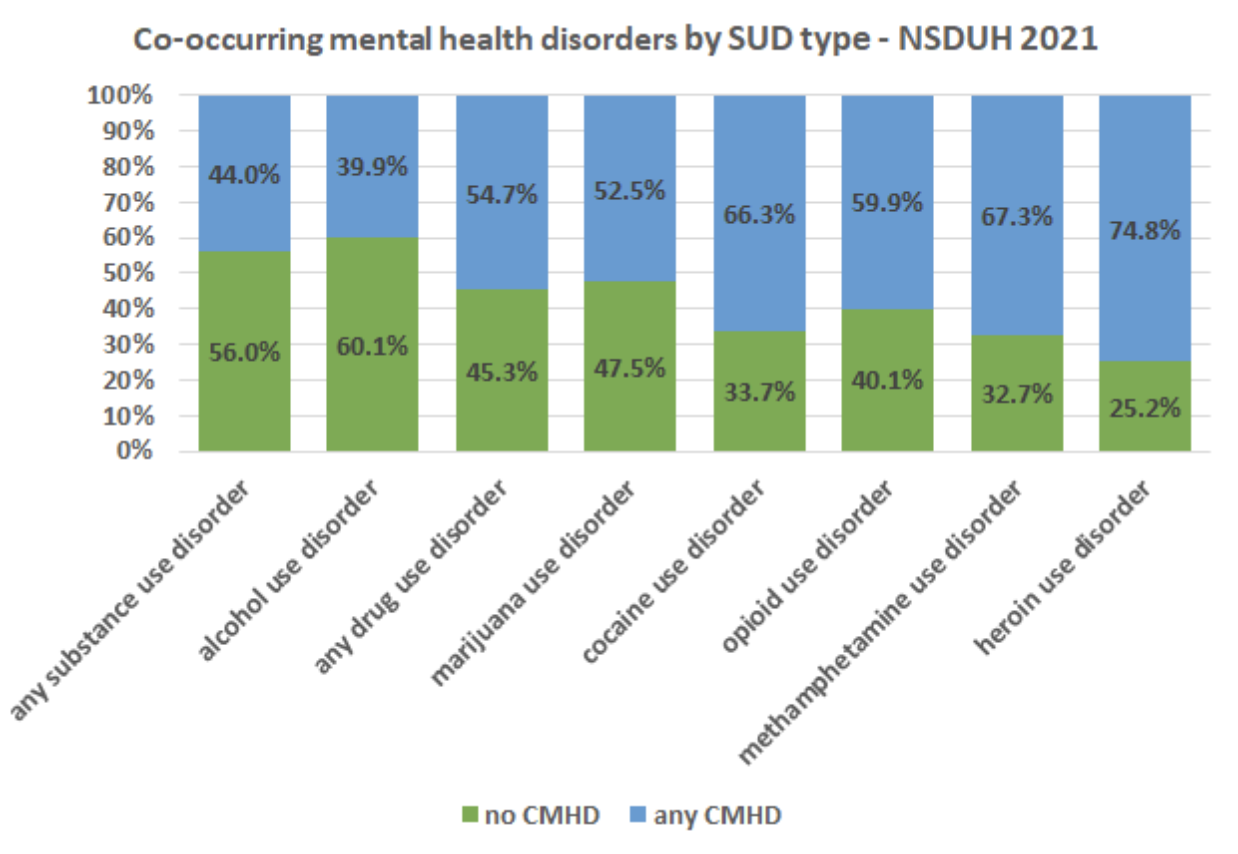
Although drugs’ chemical differences might have some effect, it would be a mistake to emphasize this. The difference alone between heroin use disorder (75 percent CMDH) and opioid use disorder (just under 60 percent) points to the importance of other factors—such as legality, availability, cultures and stigmatization.
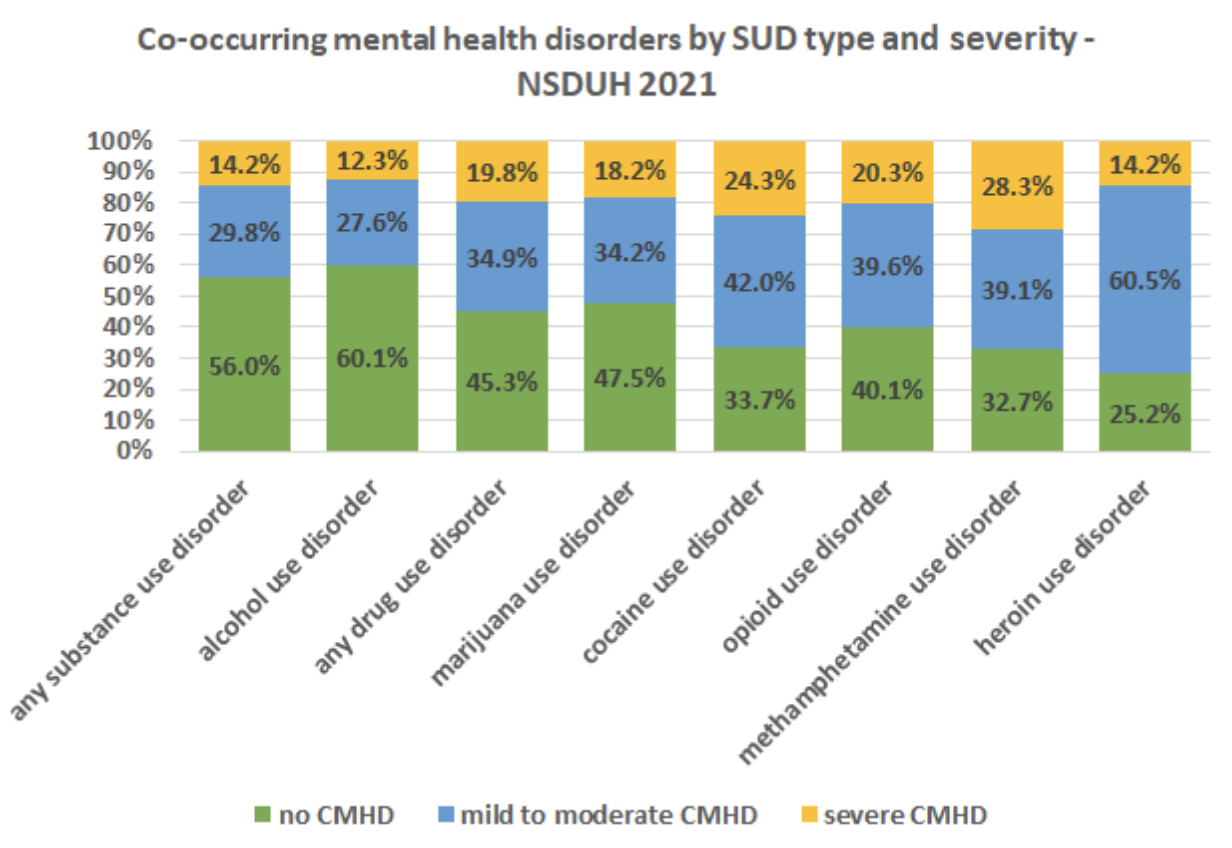
NSDUH also measures severity of CMHD. People with alcohol use disorder were found to have the lowest rate of severe co-occurring disorders: just over 12 percent. Among people with any drug use disorder, that figure was almost 20 percent. People with methamphetamine use disorder showed the highest rate, at over 28 percent.
Perhaps unexpectedly, people with heroin use disorder were found to have relatively low rates of severe CMHD, at just over 14 percent:
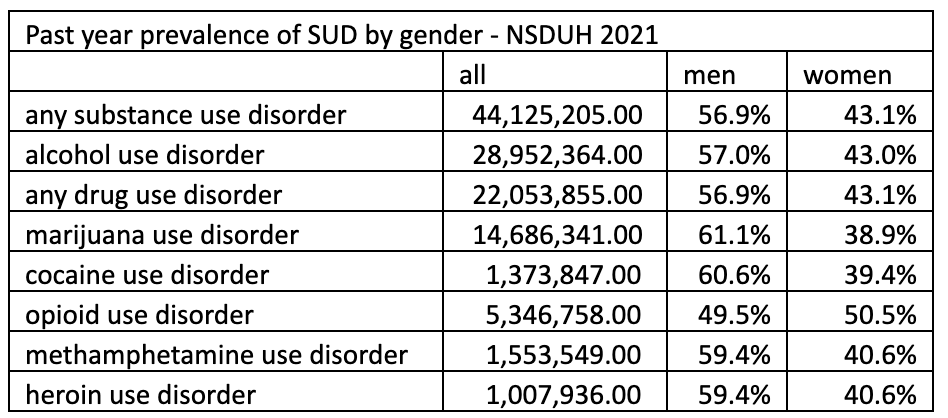
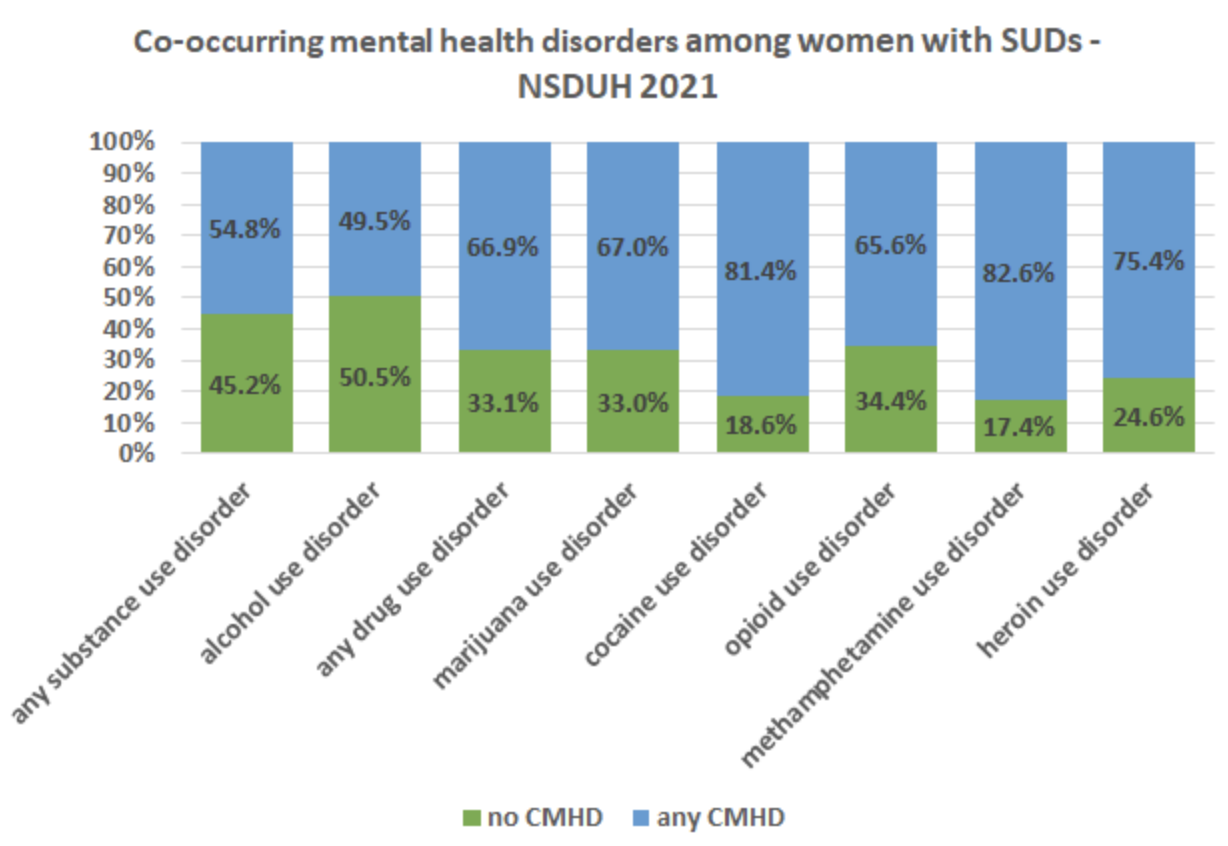
NSDUH also breaks down its figures by gender. Except for opioid use disorder, reported rates of substance use disorder are somewhat higher among men than women:
But what we see across the board—as in many other studies—are much higher rates of CMHD among women than among men.
Among women with any substance use disorder, almost 55 percent in the 2021 NSDUH survey were found to have CMHD, compared with under 36 percent of men. For alcohol use disorder, it was just under half of women versus a little under a third of men. The gender gap persisted across all substances; for methamphetamine use disorder, almost 83 percent of women were found to have CMHD:
Since all of the studies referred to in this article were cross-sectional, it is important to note that no deductions about causality can be made. The studies all asked their subjects questions about symptoms and behaviors, and diagnoses were assigned based on the answers. The questions used varied widely from study to study, which may help explain why prevalence estimates also sometimes varied greatly.
Alvaro Castillo-Carniglia et al. published a 2019 paper which reviewed the research on CMHD in people with alcohol use disorder (AUD). According to this paper, 16 studies found co-occurring antisocial personality disorder in people with AUD. But the studies differed wildly in their estimates of the percentages—ranging from 1-56 percent, with a median value of 18 percent. Seven studies, also addressing AUD, looked at co-occurring borderline personality disorder: Their figures ranged from 6-66 percent, with a median value of 21 percent.
One study found major depressive disorder in 37 percent of people who’d had a diagnosis of alcohol use disorder at some point in their lifetimes. In people with a diagnosis of AUD in the past year, rates of major depressive disorder ranged from 4-22 percent across several studies. One study also found the prevalence of ADHD in adults with current AUD to be 33 percent.
Regarding anxiety, the ECA survey found that 19.4 percent of people with AUD had had a diagnosis of some type of anxiety disorder in their lifetime.
Meanwhile, the National Comorbidity Survey (NCS), conducted from 1990-1992 with about 8,000 subjects, found that 8.6 percent of men with AUD had had a generalized anxiety disorder diagnosis at some point in their lives; for women, it was 15.7 percent. For diagnoses of panic disorder, the numbers were 3.6 percent for men and 12.9 percent for women. For social phobia diagnoses, it was 19.3 percent for men and 30.3 percent for women.
The NCS survey also looked at PTSD, finding that among women with AUD, 26.2 percent had a PTSD diagnosis at some point in their lives, compared with 10.3 percent of men.
Substance use treatment providers must never assume they know best about their clients. People are the experts on their own lives.
The ECA survey found schizophrenia in 3.8 percent of people with AUD (the prevalence of schizophrenia in the general US population is estimated at between 0.25-0.64 percent). Bipolar disorder was found in 3.5-5 percent of people with a diagnosis of AUD at some point in their lives.
Finally, a 2020 paper by Elizabeth A. Evans et al. measured CMDH among people with a diagnosis of opioid use disorder (prescription or heroin) at some point in their lives, and found the following: PTSD (35.5 percent of women and 17.4 percent of men); major depressive disorder (women 59.6 percent, men 42.0 percent); anxiety disorder (women 54.6 percent, men 30.8 percent); and personality disorder, such as borderline, antisocial, etc. (women 55.1 percent, men 57.0 percent).
Very importantly, broad figures like all of these undoubtedly disguise much greater concentrations of CMHD in specific populations. Gabor Maté worked with unhoused people with heroin use disorder in Vancouver’s Downtown Eastside, and it is not surprising that he found very high rates of co-occurring trauma and PTSD.
However, Maté’s sample doesn’t generalize to all people with substance use disorders.
People with PTSD or other co-occurring disorders deserve treatment, and sadly they too rarely get it. But people with substance use disorders who do not have PTSD will not be helped by PTSD treatment, and may even be harmed by it.
All of which is to say that substance use treatment providers must never assume they know best about their clients. People are the experts on their own lives. How do we best match substance use treatment to the individual? The first step is to ask the person what they want.
*Percentages were calculated using SAMHSA’s online Public-use Data Analysis System (PDAS). The following variables were used:
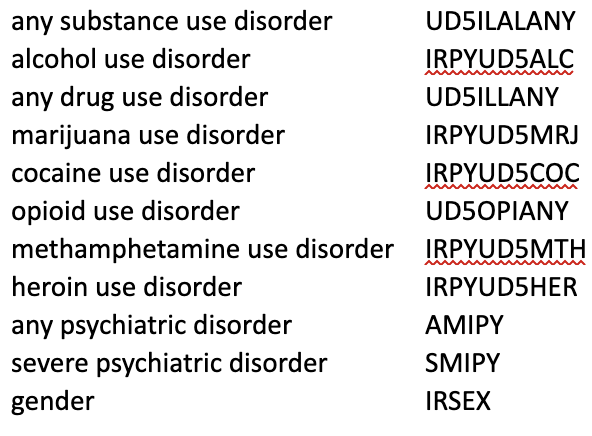
Photograph by Stefano Pollio via Unsplash. Graphics by Kenneth Anderson.



