Opioids like heroin and fentanyl have grabbed the media and legislative spotlight—from soaring overdose fatalities to the misguided prescription restrictions and drug-induced homicide laws ostensibly intended to combat them. What’s glossed over is that our overdose crisis primarily relates to polysubstance use. Around 80 percent of deaths involving a synthetic opioid in 2016, for example, also involved another drug. When we only focus on partial data, we only come up with partially effective solutions. With our cultural narrative failing to acknowledge this, people who use drugs need to make the effort to learn more to keep ourselves safer.
Most forms of polysubstance use carry potential negative effects and risks. Mixing uppers and downers—whether using one drug to come off of another, or intentionally creating a “speedball” effect —presents a unique set of challenges to your body. It can be deadly.
Super-potent fentanyl showing up in illicit drug supplies in many places across the United States and being taken unwittingly by consumers of heroin, meth and cocaine is obviously a big factor. But other areas, such as Denver, where I work in a syringe exchange, are seeing heightened overdose rates without significant presence of fentanyl in their supply. Mixing other drugs with plain old opioids is commonly the culprit.
Many people have started to shift the narrative to include stimulant-involved overdoses (or “overamping”). Fewer emphasize the role of benzodiazepines—typically when mixed with opioids or other depressants like alcohol. Part of the reason is that benzos are commonly prescribed and therefore wrongly assumed not to involve risks. Yet over 30 percent of opioid-related overdoses also include benzodiazepines. One study published this year showed that using benzos with opioids increases overdose risk five-fold compared with using opioids only.
An Intro to Benzos
Benzodiazepines are often prescribed to combat acute anxiety and panic as well as longer-term anxiety disorders. They include well known brands such as Xanax, Valium, Klonopin and many more. Benzos were first synthesized in the 1950s and introduced to the US medical market in the ‘60s. They quickly became popular as replacements to barbiturates (which were associated with the deaths of Marilyn Monroe, Elvis, Jimi Hendrix, John Belushi and many other stars). By 1999, 8.1 million prescriptions for benzos were written annually in the US; by 2013, that number had increased to 13.5 million.
It’s important to note that benzos on their own can absolutely be used safely. Even when taking over the prescribed or recommended limits, people who use benzos are most frequently at risk of blacking out, poor judgement and sleep—as opposed to the respiratory depression associated with potent opioids.
However, this risk assessment changes drastically when multiple substances are used at once—or even with overlapping effectiveness intervals. Many people do not account for taking their anxiety medication in the afternoon with an evening of binge drinking on the horizon, for example. Consuming strategically can be a lifesaver.
As with any drug, general harm reduction guidance for benzos includes:
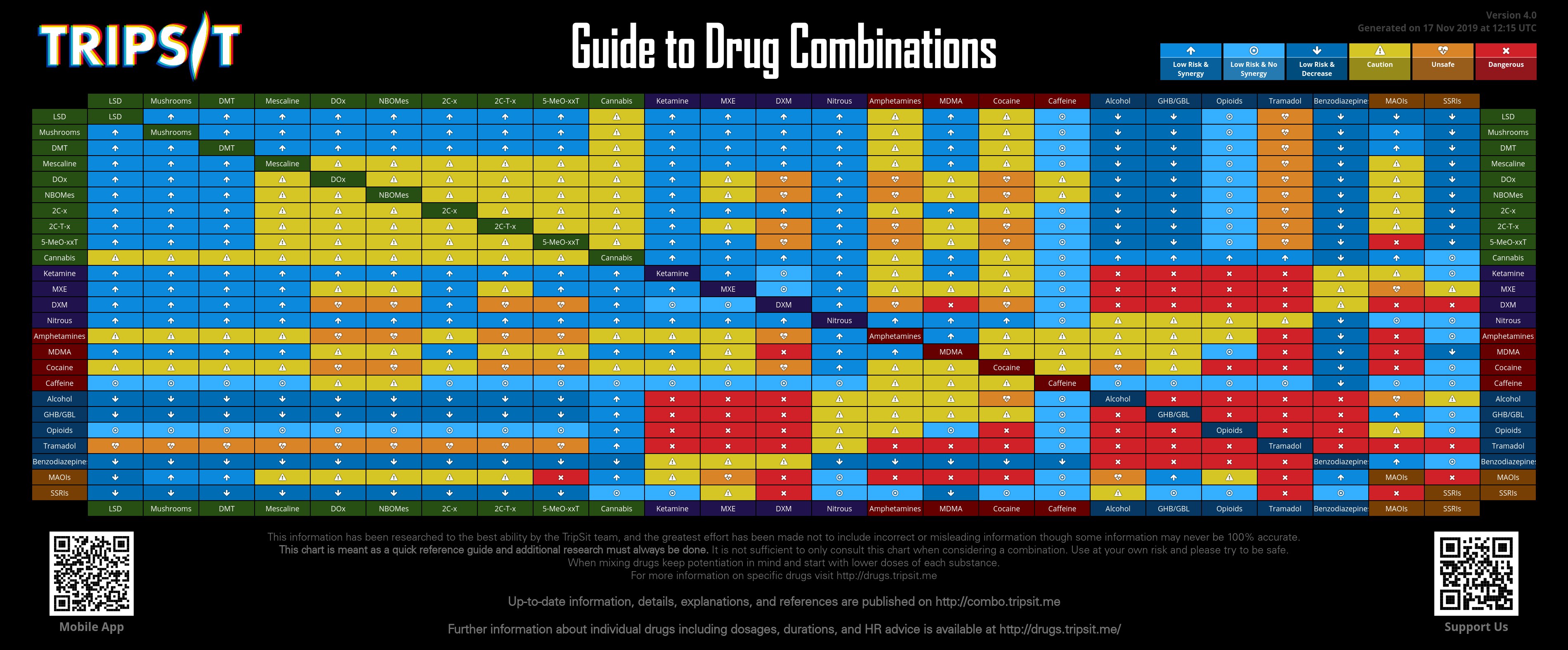
*avoiding high-risk combinations—above all, mixing benzos with alcohol, GHB or opioids
{kind=link}
*avoiding situations that present heightened danger (e.g, driving while on high doses)
*setting personal boundaries to avoid excessive or compulsive redosing
Reducing the Risks of Pressed Pills
Many doctors have become increasingly hesitant to prescribe benzodiazepines over the last decade. And like many formal or informal restrictions, this has unintended consequences: People pursuing the anxiety-suppressing, sedative and disinhibiting effects of benzos may have to turn to the streets to obtain their supply, and illicit production and distribution of similar substances without oversight increases.
We have seen this play out with heroin, for chronic pain patients refused opioids, and we’re watching it unfold with benzos. Unregulated benzos, like other “street” drugs, can contain fentanyl and many other dangerous substances. Having naloxone on hand and knowing how to use it is always a good idea, even if you’re not intending to use opioids.
Demonizing “pressed” pills won’t help, however. People seek street benzos as a response to lack of access to needed medication. But without fueling media panics around “fake” Xanax and other pressed pills, we need to look calmly at practical ways to reduce risk for people who use them. Not all pressed pills are created equal—quite the opposite—and understanding what you’re ingesting is paramount.
When obtaining benzos at street level—including at a friend’s house—it’s always good to know the source. If you don’t know for certain that a doctor has prescribed the pills you intend to ingest, here is a non-exhaustive list of ways to identify a pressed pill:
*An asymmetrical shape
*Inconsistent thickness
*No waxy covering
*It has a chalky consistency, and dissolves or disintegrates when held
*It lacks a bitter taste when consumed
These checks are imperfect, however. Some pressed pills may seem pharmaceutically produced in every way.
Some pills are manufactured to contain fentanyl or fentanyl analogues and are sold as such. Others are manufactured in facilities where fentanyl is present, and cross-contamination occurs due to lack of oversight and proper hygienic practices. Regardless of intent, if you spot a pressed pill or don’t know the origin of any pill you intend to ingest, checking a chunk of it—using resources such as those offered by Dancesafe—is a potentially lifesaving strategy.
It’s also important to note that if a pressed pill does contain the correct substance, the dosing may still not be homogenous (evenly distributed across the pill), and it may contain more or less of the substance than anticipated. So if you’re splitting a bar of “Xanax” that hasn’t been produced with homogeneity testing, there is a high likelihood of unknown dosing. Starting by ingesting a smaller amount than you think you want is an obvious harm reduction step.
Combinations, Dependence and Withdrawal
If you’ve decided that you want to use benzodiazepines in combination with any other drug, another important harm reduction tactic is taking the other drug first if possible (granted, this is complicated when many people need benzos to function through debilitating panic, anxiety and trauma-related disorders).
This is because benzos lower inhibitions (the same applies to alcohol). Once under their influence, it can be easy to decide to take more of another drug than you intended, heightening the risks of the combination. If you intend to mix opioids and benzos despite the risk, do your heroin or other opioid first. Then see if the benzos are necessary. Taking the opposite approach frequently results in death.
Many people also experience dependence to benzos. Ways to increase your chances of a non-problematic relationship with them include: understanding that all drug use exists on a spectrum; drawing amount- or time-related boundaries around your use when possible; and considering using different drugs on different occasions, rather than constantly using benzos.
Finally, it’s also vital to know that cessation of benzodiazepine use at high dosing can quickly turn deadly. Understanding a tapering regimen, in which someone slowly reduces the amount of drugs they’re taking to avoid drug-induced seizures, is important. Seeking proper medical advice, when possible, is always advisable.
Keeping Sight of the Bigger Picture
Beyond this elementary introduction to benzodiazepines, we also need to address the larger issues at hand: an uninformed populace in an unequal society, vying desperately to numb daily or past trauma and anxiety with no access to honest drug education, is a recipe for an endless overdose crisis.
People scared of losing health insurance and support are incentivized not to be honest to health professionals about their consumption of non-prescribed drugs, and therefore less likely to be given the information they need to keep themselves safer.
We must reduce the stigma attached to consuming drugs in prescribed and non-prescribed contexts, and treat people with problematic drug relationships with compassion, arming them with knowledge and resources to protect themselves. The alternative is to continue to lose those we love to preventable drug-related deaths.
Like this article? As a nonprofit publication, Filter is funded entirely by donations and grants. If you wish to support our work of reporting on drug use, drug policy and human rights, please donate using the button below. We’re so grateful for your support.
This article has been amended to reflect the fact that over 30 percent of opioid-related overdoses also include benzodiazepines. An earlier version initially stated that the 30 percent figure applied to opioid-related deaths.
Image via: Medicine for the People