The members of the American Association for the Treatment of Opioid Dependence (AATOD) are outraged. This national organization represents the interests of over 1,200 opioid treatment programs (OTPs), also known as methadone clinics. The group’s anger was triggered by two bills: the Opioid Treatment Access Act (OTAA), which the group labels as “dangerous,” and the Mainstreaming Addiction Treatment (MAT) Act. Each bill recommends a few modest changes to loosen restrictions on access to methadone and buprenorphine.
To kill the bills, the group created fact sheets that are full of misleading statements, exaggerations and lies of omission, as well as being condescending to people who take methadone.
According to Mark Parrino, founder and president of AATOD and a former clinic owner, the group began circulating these documents three months ago, giving them to state member chapters and “a number of congressional staff members.” He told Filter, “They were written through our legislative committee membership as a way of expressing our concern about two pieces of legislation.”
Members sense a direct threat to their power and profits.
The misinformation in the documents is shocking from an organization that purports to believe in “evidence-based clinical practice.” AATOD went ballistic over a provision in the OTAA that allows a small group of board certified physicians outside of OTPs to prescribe methadone, with pharmacy pick-up. Members sense a direct threat to their power and profits. Clinic owners prefer the status quo that has given them cartel-like control over methadone for over 40 years.
The OTAA fact sheet goes off the rails by insinuating that relaxing rigid clinic regulations and licensing outside doctors to prescribe methadone would exacerbate the overdose crisis: “It will result in physicians prescribing a powerful medication with no effort to limit diversion, no counseling, no drug testing … exactly how we got into the current opioid epidemic and record numbers of deaths.”
In fact, it’s the opposite. The OTP system is partly to blame for the massive increase in overdose deaths, because it’s still easier to get fentanyl on the street than it is to get into and stay in a methadone program. Methadone is proven to cut the death rate for people with opioid use disorder (OUD) by 50 percent or more, but not if you can’t get it.
Like the DEA itself, AATOD always invokes “diversion”—the notion of people giving or selling their medications to others—to block reform.
“Spotlighting diversion when we know that methadone (diverted or otherwise) is the best tool to stem the worst overdose crisis in American history is the wrong move,” Aaron Ferguson, a methadone liaison with the Urban Survivors Union, told Filter. “Prescribing all medications comes with a cost/benefit analysis of treatment compared to none at all, and methadone and people who use drugs are no exception to this general rule of health care.”
ATTOD’s insistence that counseling is necessary for methadone patients is also false. A National Academy of Sciences, Engineering, and Medicine Consensus report concluded in 2019 that methadone treatment should not be contingent on the availability of other services. The real reason for AATOD’s position? Counseling is a billable service.
“I need methadone to live a normal life but I feel doomed every day.”
“I am still frustrated to have to participate in coerced talk therapy with a rotating cast of counselors to get my medication,” one methadone user told Filter. Another person shared her exasperation with me privately: “What really blows my mind is that people can go buy guns, guns that can kill people and just have them forever. No daily, weekly, monthly, yearly check-in. No drug tests, no fucking mandatory counseling sessions with a new college graduate every other month. I need methadone to live a normal life but I feel doomed every day.”
Mandatory counseling is an oxymoron, and is unethical because of the huge power imbalance between patient and counselor. For example, if a person reveals use of an illicit drug or a urine screen is positive, their counselor has the authority to revoke take-home bottles, cancel a vacation or subject them to “administrative discharge”—i.e. kick them out of the clinic. Missing a counseling session can also result in sanctions. It is outrageous and unacceptable that counselors have this power over patients’ lives. No true therapeutic alliance can be built in these excessively punitive and coercive circumstances.
AATOD refuses to acknowledge that clinic-generated barriers to care are killing people. OTPs’ culture of cruelty, as described in the Methadone Manifesto, sees their punitive policies literally drive people out of treatment, putting them at great risk of fentanyl-involved overdose. Almost half of people with OUD are not retained in treatment at 12 months, and this rate reduces further over time.
AATOD’s fact sheet also attacks pharmacy-based dispensing, like that seen in the UK and Canada. It warns: “Suggesting that methadone is safe and effective for OUD in any other setting [other than an OTP] is scientific appropriation: it is not evidence-based.”
This is another misleading statement. The efficacy of pharmacy-based methadone prescribing is evidence-based. This low-threshold model has been in existence for over 40 years. It doesn’t create obstacles to getting medication or trigger NIMBY protests. It has excellent retention rates, and mitigates stigma.
The fact sheet wrongly asserts that pharmacists in Scotland and England don’t supervise methadone consumption. They do. To be sure, no system is perfect, but picking up a prescription of methadone at a local pharmacy makes a lot more sense than the current, outdated OTP model, especially during an ongoing overdose crisis and a pandemic.
“To circulate a document so out of step with the medical and scientific consensus raises questions about AATOD’s motivations and leadership.”
People who take methadone have been screaming this into the void for decades, but ATTOD hasn’t been listening. A recent study conducted in the US demonstrated the desire for liberation from the clinic system. Study participants who received methadone at a pharmacy reported high rates of satisfaction and endorsed the statement, “Pharmacy is the right location for receiving methadone for MMT.”
“To circulate a document so out of step with the medical and scientific consensus raises questions about AATOD’s motivations and leadership,” Dr. Paul Joudrey, an assistant professor at the University of Pittsburgh School of Medicine told Filter. “They cannot cherry pick the science just because they don’t want things to change. They should listen to expert groups like the National Academy of Science and Medicine and put patients’ needs first.” Joudrey has written a point-by-point refutation of the AATOD fact sheets.
Parrino pushed back on some of the criticism of the fact sheets. He told Filter he opposes prescribing methadone for OUD outside clinics because, “It’s important to underscore the fact that methadone maintenance treatment as used in an OTP… uses a team approach, not a singular practitioner approach in dealing with opioid use.” A safety concern he raised with office-based prescribing was use of prescription drug monitoring programs. “A majority of practitioners do not check the PDMP when other practitioners are prescribing opioids including methadone for pain management.”
As for therapy, he argued, “The claim is that counseling really doesn’t do much to enhance the use of the medication. This conclusion was based on limited studies with a small patient population. It is also an attempt to marginalize more than 60 years of evidence-based research that demonstrates patient outcomes do improve.” Parrino cited a dated study published in 1988 to make this point.
AATOD’s attack is a response to unprecedented changes to methadone regulations that occurred during the pandemic. COVID-19 cracked open the clinic system in a way nothing else has. This revealed a number of facts that are inconvenient for AATOD—and which are nowhere to be found in its fact sheets.
The Substance Abuse and Mental Health Services Administration (SAMHSA) emergency guidelines permitted clinics to give more take-home bottles of methadone; normally it takes months or even years to “earn” an increase. To reduce the spread of the coronavirus, weekly drug screening was eliminated in some clinics, as was mandatory group counseling. Thousands of patients were freed from rushing to a clinic six days a week, from urine testing and from counseling sessions that are often a waste of time.
So what happened? The sky didn’t fall, nor did diversion or overdose rates increase. Numerous studies conducted during the pandemic back this up: There were very few incidents of diversion and allowing more take-home bottles didn’t increase overdose deaths. One study concluded, “Despite a near-doubling of take-home methadone doses during the COVID-19 exemption period, the increase in take-home doses was not associated with negative treatment outcomes in methadone-adherent clients.”
Another study, just published by researchers at the National Institute on Drug Abuse (NIDA), also found that OTP take-home policy changes didn’t increase overdose deaths and stated, “Coupled with research demonstrating improved patient satisfaction, treatment access, and engagement from these policies these findings can inform decisions about permanently expanding take-home methadone.”
This new research is good news for people who take methadone but bad news for AATOD, because these studies conclusively debunk its bogus claims.
“There’s a group of people that just don’t want to go to a methadone clinic … How do we address this?” asked NIDA Director Dr. Nora Volkow recently. Some of the answers were staring her in the face.
Parrino’s response to the new research was tepid: “It’s true that the COVID-19 pandemic gave OTPs the opportunity to provide greater amounts of take-home medication. Much has been made about the fact that there were not resulting overdoses and methadone diversion. That is true to a point. The more hidden story is that the OTPs were always monitoring how the patient was using take-home medication, even during the early period of March 2020 to September 2020 when toxicology reports were not being collected to further protect the patients and staff.”
All of this new research is good news for people who take methadone but bad news for AATOD, because these studies conclusively debunk its bogus claims. OTPs are freaking out because for the first time their fucked up, carceral system is under a microscope. They’re apoplectic that groups of methadone users, health care providers, researchers, politicians and policymakers are coming together to challenge their hegemony.
“What is certain is that the increasing overdose rates is unacceptable, and our system does need to improve in terms of its integration and in terms of its overall guidance in treating this disorder,” Parrino said.
The profit motive permeates the OTP-industrial complex.
So why is AATOD trying to defeat legislation that will save lives? AATOD is doubling down and balling up its fists to fend off any reform that doesn’t center the clinic system. The profit motive permeates the OTP-industrial complex—from drug testing to video surveillance systems to counseling to attendance requirements. Follow the money. They want patients to come to the clinics six days a week and not get 14 or 28 day take-homes, because in order to make bank they need to bill insurance or patients for every single visit. More take-home bottles mean less cash flow. Investors in for-profit clinics—BayMark Health Services has estimated annual revenue of $86.7 million—don’t like that!
The clinic wardens of AATOD love the carceral structure of OTPs that keep patients vulnerable and subordinate, because it ensures that few can “earn” their way out. Cha-ching! The prospect of doctors prescribing methadone in primary care or other non-OTP settings is a mortal threat to AATOD’s existence and they will attempt to prevent it by any means necessary, including lying and scaremongering.
AATOD’s “factless” fact sheets are just an opening salvo. The organization is well-funded, has decades of lobbying and legislative experience at the state and federal levels, and deep connections to the DEA and SAMHSA. They will not take off the “liquid handcuffs” and let the prisoners go without a fight.
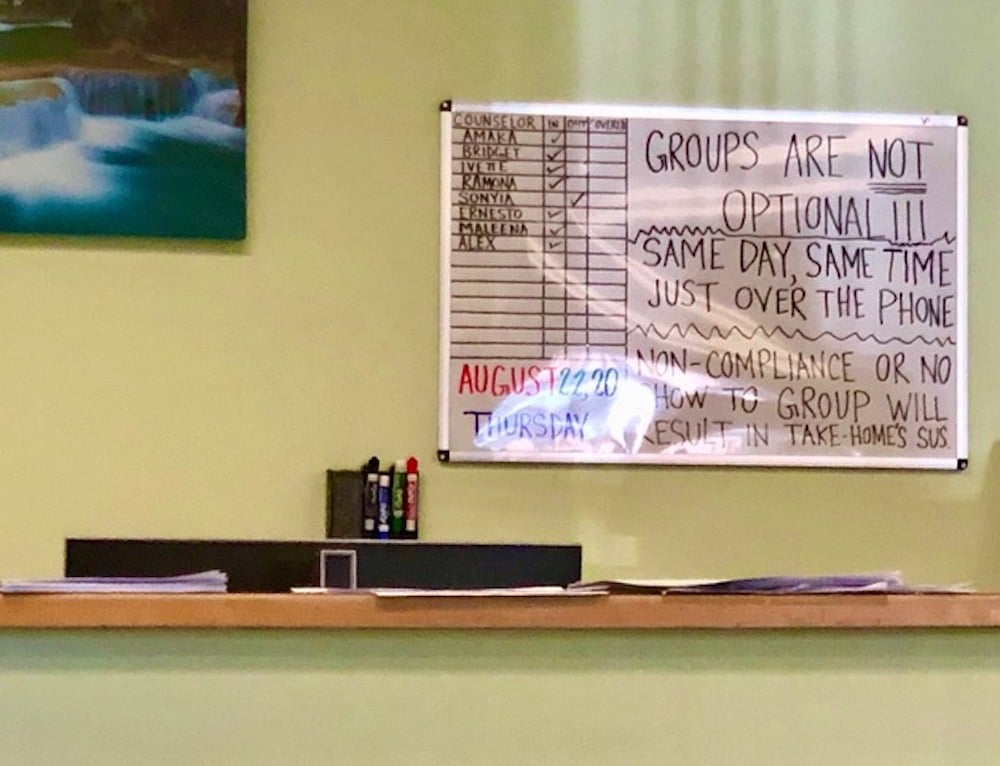
Photograph of a sign at a methadone clinic, reading “Groups are not optional … Non-compliance or no show to group will result in take-home [suspension],” by Helen Redmond




Show Comments